
Arthroscopic treatment of a femoral osteochondroma as a cause of femoroacetabular impingement. A case report
Tratamiento artroscópico de un osteocondroma femoral como causa de choque femoroacetabular. A propósito de un caso
Introduction
Osteochondroma is a benign overgrowth derived from an aberrant subperiosteal germ composed of bone and cartilage that grows and maturates through normal enchondral ossification. These lesions manifest as isolated tumour lesions in 90% of the cases(1), and are only rarely observed in the context of multiple exostoses. Osteochondromas are mainly located in the metaphyseal zones of the long bones, basically the distal femur, the proximal humerus and the proximal tibia(1,2). Their location in the femoral neck is exceptional(3).
The clinical presentation of femoral neck osteochondromas depends on their size and specific location. They may give rise to mechanical restriction of mobility, with pain secondary to a mass effect or to the compression of nervous or vascular structures.
A number of publications can be found referred to the arthroscopic resection of osteochondromas of the femoral neck(4,5,6,7), though most correspond to clinical cases or series involving only a few cases. In some cases, as a consequence of their size and location, these lesions give rise to symptoms secondary to impingement between the different joint structures.
The present case corresponds to a young woman with a femoral neck osteochondroma, in which arthroscopic resection of the deformity was carried out. A brief review is made of the current literature, with few similar cases being found to date.
Clinical case
We present the case of a 49-year-old woman with left hip pain and limping for approximately two years. Her history indicated surgery of the hip in adolescence, though the cause of surgery was not known, and no documentation was available. The physical examination revealed pain in response to flexion and internal rotation of the hip, with positive anterior impingement manoeuvring. The plain X-rays (Figure 1) showed large, isolated exostosis in the femoral head-neck transition zone, with no evidence of associated exophytic lesions. The magnetic resonance imaging study revealed exostosis of the anterolateral surface of the femoral neck, measuring 21 × 14 mm in diameter (Figure 2), with signs suggestive of rupture of the anterosuperior labrum.
reacae.29377.fs2205007en-figure1.png
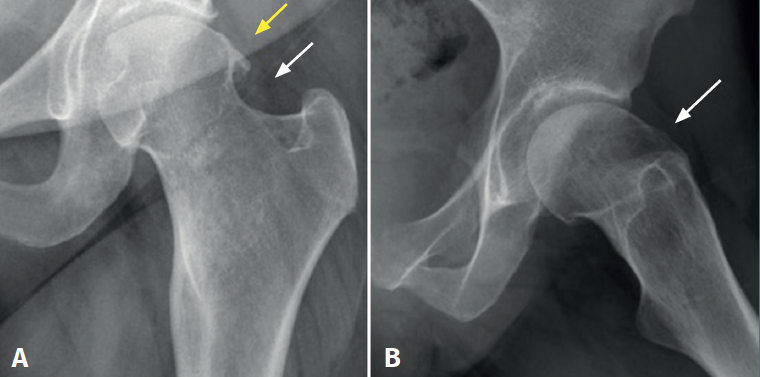
Figure 1. A: anteroposterior plain X-ray view of the left hip, showing exostosis of the femoral head-neck transition zone; B: axial plain X-ray view of the left hip, showing exostosis of the femoral head-neck transition zone.
Surgery consisted of arthroscopic removal of the exostosis and debridement of the labral lesion using an inside-out technique(8). In a first step we evaluated the peripheral compartment, identifying a large exophytic tumour (Figure 3) located in the anterolateral zone of the femoral neck. Two samples of the tumour were obtained for histopathological study (Figure 4), and labral debridement with arthroscopic resection of the tumour was carried out (Figure 5). In addition, loss of cartilage thickness of the femoral head was noted. Evaluation of the central compartment was carried out in a second step, following resection of the exostosis, revealing chondral degeneration zones.
reacae.29377.fs2205007en-figure2.png
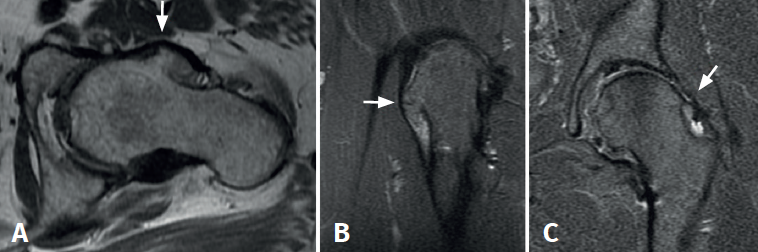
Figure 2. A and B: magnetic resonance imaging (MRI) axial view in T1 sequence (A) and coronal view in T2 sequence (B), revealing a large exostosis on the anterolateral surface of the femoral neck; C: coronal view in T2 sequence showing exostosis of the femoral neck and signs consistent with anterosuperior labral rupture.
The postoperative radiographs (Figure 6) showed complete resection of the tumour, with correct joint congruence. The pathology findings were consistent with osteochondroma (Figure 7). The clinical course was favourable during the first year, with weight bearing using crutches for 6 weeks, followed by physiotherapy. The symptoms subsequently reappeared, with mechanical pain in the inguinal region that increased in intensity with rotation and caused limitation of her daily activities - the Harris Hip Score being 34 points out of 100. A new magnetic resonance imaging study revealed femoroacetabular impingement and thinning of the joint cartilage (Figure 8). A total hip arthroplasty was therefore proposed and carried out 18 months after arthroscopic resection of the osteochondroma. The femoral head was sent for histopathological study, which confirmed the existence of residual osteochondroma (Figure 9).
reacae.29377.fs2205007en-figure3.png

Figure 3. A: arthroscopic view of the peripheral compartment from the anterior portal, showing the tumour of the femoral neck; B: arthroscopic view of the peripheral compartment from the anterolateral portal, showing the tumour (highlighted by a broken line) of the femoral neck.
Discussion
The described case corresponds to a neoformative lesion in an infrequent location. Despite the benign nature of the process, its location generated symptoms secondary to the femoroacetabular impingement. Given the size and location of the lesion, an arthroscopic approach was considered to be feasible.
reacae.29377.fs2205007en-figure4.png
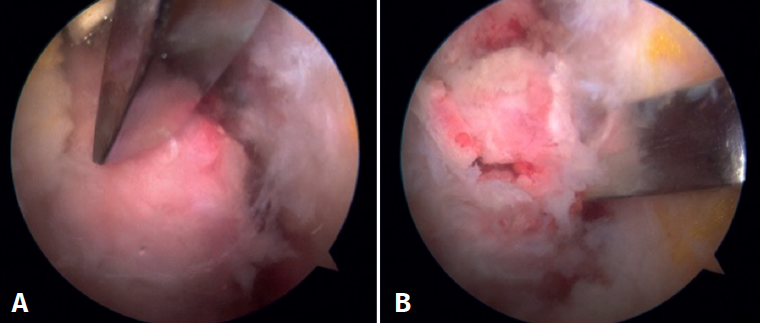
Figure 4. Arthroscopic view of the peripheral compartment from the anterior portal, corresponding to different moments of biopsy sampling with the 5-mm osteotomy.
Osteochondromas are the most common primary benign tumours of osteocartilaginous origin(9). They account for 36% of all benign bone tumours and 8.5% of all bone neoplasms(10). They are considered to be very infrequent in the proximal femoral zone. In the hip, the symptoms are variable and are conditioned by the location and size of the lesion. The tumour may constitute a casual finding or can cause a range of symptoms such as pain, nerve irritation(11) or tendon prominences(12). In our patient the main symptom was pain predominantly upon flexion and internal rotation, secondary to impingement of the lesion against the labrum.
reacae.29377.fs2205007en-figure5.png
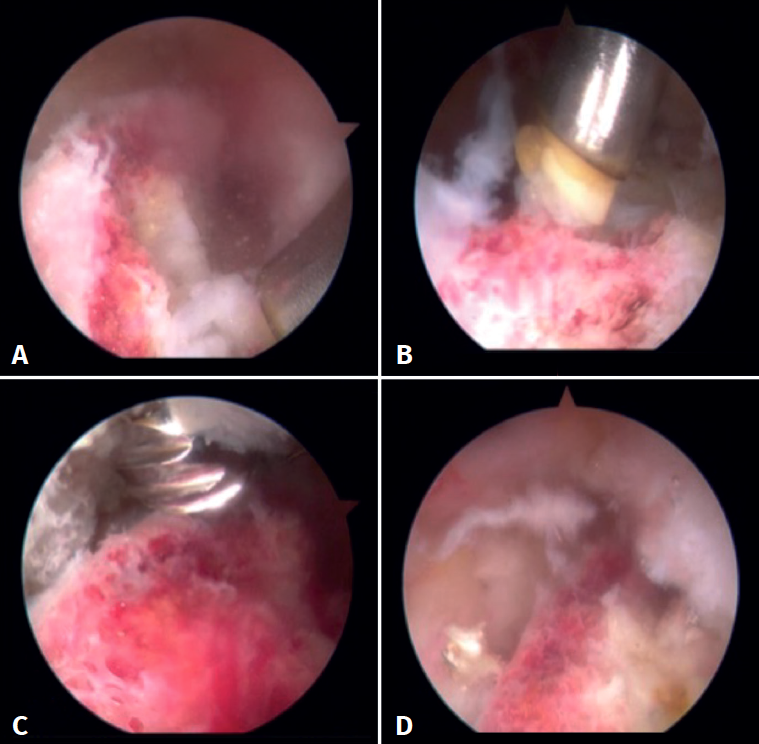
Figure 5. Arthroscopic view of the peripheral compartment from the anterior portal, corresponding to different moments of radiofrequency individualisation and tumour resection using a 4-mm round bur.
Despite the infrequent location in the femoral neck region, a number of cases similar to our own can be found in the literature. Different studies describe removal using open techniques, such as the case series published by Sieberonck and Ganz(13), describing resection via subluxation of the femoral head in four patients, with no case of associated osteonecrosis.
reacae.29377.fs2205007en-figure6.png
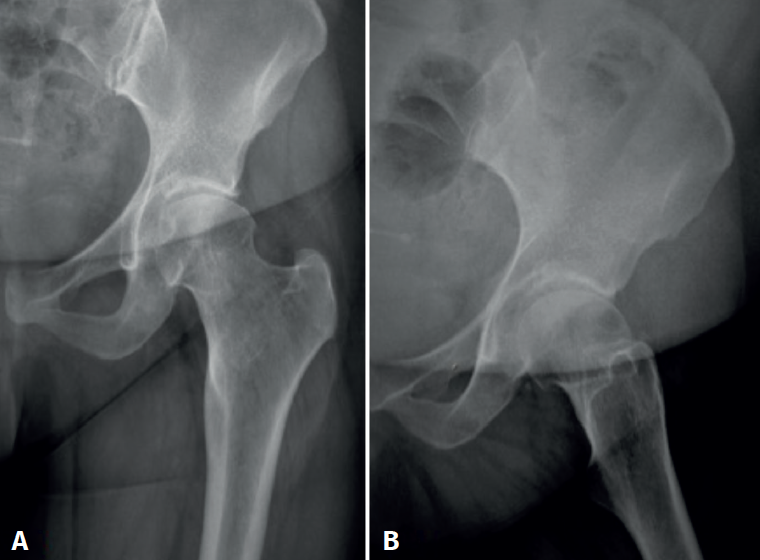
Figure 6. A: anteroposterior plain X-ray view of the left hip, following arthroscopic resection of the tumour; B: axial plain X-ray view of the left hip, following arthroscopic resection.
Recently, Hammad et al.(14) have described open resection via a posterolateral approach in the case of a large osteochondroma. In such cases the authors advocate prophylactic fixation of the femoral neck using cannulated screws, due to the risk of fracture and secondary necrosis.
reacae.29377.fs2205007en-figure7.png
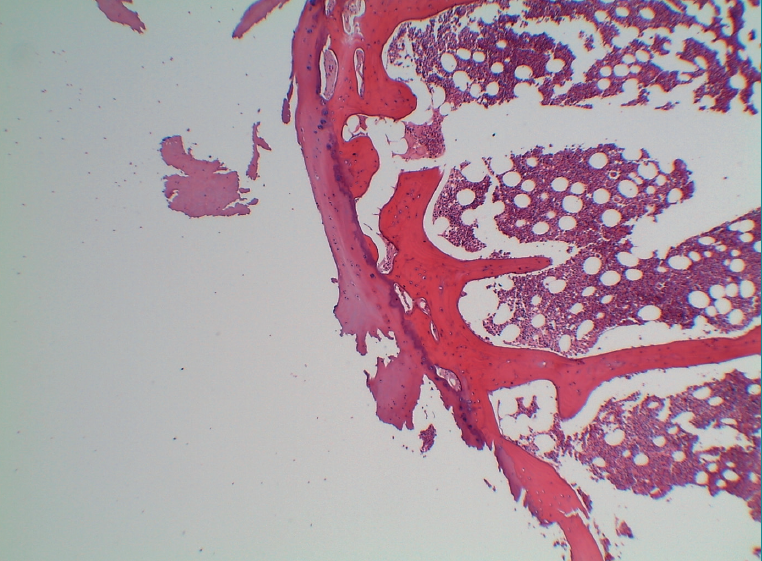
Figure 7. Histological view of the sample, showing a peripheral capsule of mature cartilage, chondrocytes with a small nucleus and vacuolated cytoplasm, no signs of atypia, and showing enchondral ossification with preserved trabeculae, in the context of signs of haemorrhage and mild chronic inflammation (HE, x4 magnification).
The first case of arthroscopic resection of an osteochondroma of the femoral neck was described by Feeley and Kelly in 2009(5), and they also described an associated labral lesion such as that seen in our patient. On the other hand, Aguiar and Dantas(7) in 2014 published the first two cases of osteochondroma of the femoral neck resected via arthroscopy and of a larger size than the lesion described by Feeley. In both cases, these authors used an outside-in technique to evaluate and treat the lesions of the peripheral compartment first, showing the cause of femoroacetabular impingement to be the tumour. In this same line, in 2016, Sharfman et al.(6) published three cases (2 enchondromas and 1 osteochondroma) subjected to arthroscopic resection, with good results. Another clinical case similar to our own was published by Wang et al.(3) in 2017. In contrast to our case, these authors described a lesion located in the posteroinferior portion of the femoral neck; despite this location, arthroscopic resection could be performed. In addition, their patient presented associated osteochondromatosis with multiple free bodies; these were therefore removed in the same surgical procedure. Lastly, in 2019, Alter et al.(15) published a new arthroscopic technique combining a T-capsulotomy to improve vision and facilitate resection with posterior capsular closure using anchorings and sutures to thus avoid instability. According to these authors, although the arthroscopic approach affords excellent vision particularly in locations of difficult access, it is technically demanding, and the sutures used for capsular closure may damage the joint surface.
reacae.29377.fs2205007en-figure8.png
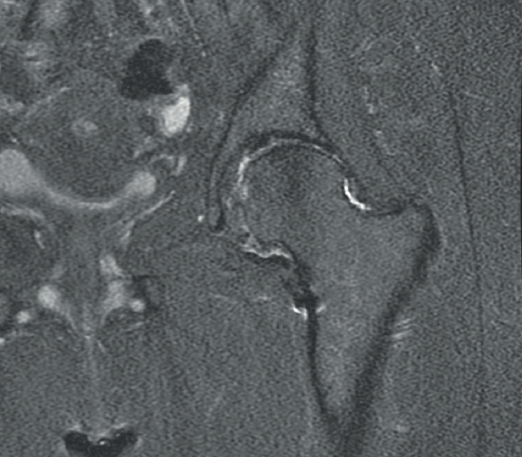
Figure 8. Coronal magnetic resonance imaging view in T2 sequence showing decreased joint cartilage and impingement of the femoroacetabular space.
With regard to the surgical technique used in our case, we usually employ the outside-in sequence in the same way as Aguiar and Dantas(7). This allows us to first evaluate the peripheral compartment and resect the tumour, and affords better access to the central compartment for treating the associated lesions. On the other hand, we performed an interportal capsulotomy, used 4-mm Wissinger rods to distend the capsule, and achieved good visibility of the lesion without needing the transverse expansion used by Alter(15), nor the posterior capsular suture. Nevertheless, we believe that this may be a useful associated manoeuvre in some lesions of greater size or involving a more complicated access.
reacae.29377.fs2205007en-figure9.png

Figure 9. Sample of the femoral head sent for pathology study in the arthroplasty procedure, showing the zone resected in the previous surgery and the loss of cartilage thickness in the anterosuperior zone of the head.
At present, it can be affirmed that there is no agreement on how to approach these lesions when they are located in the hip joint. Their size and location, and the experience of the surgical team, are the basic aspects to be taken into account in decision making. In our case, in view of the location of the lesion on the anterolateral surface of the femoral neck, and despite its large size, we chose the arthroscopic approach, considering it to be less invasive and moreover adequate for treating the associated lesions.
With regard to the labral lesion, and despite its important biomechanical role, in our case we decided against its repair using anchorings, due to the intra-substance degenerative characteristics of the lesion(16). There is evidence in the literature that alterations of the labrum may result in early degenerative disease, and this may have been one of the causes of the torpid course and outcome in our patient.
Conclusions
We consider arthroscopic resection to be the technique of choice in osteochondromas of the hip joint, provided their location and size make them approachable. In our case, and despite the coexisting joint degenerative phenomena, we chose arthroscopic management of the lesion in view of the age of the patient.
Figuras
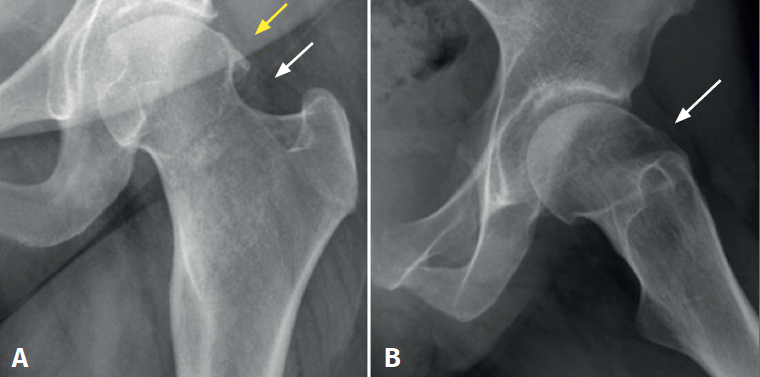
Figure 1. A: anteroposterior plain X-ray view of the left hip, showing exostosis of the femoral head-neck transition zone; B: axial plain X-ray view of the left hip, showing exostosis of the femoral head-neck transition zone.
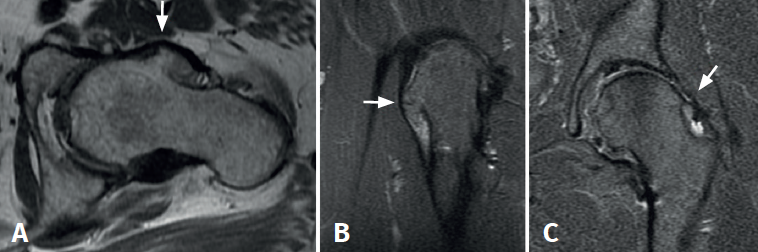
Figure 2. A and B: magnetic resonance imaging (MRI) axial view in T1 sequence (A) and coronal view in T2 sequence (B), revealing a large exostosis on the anterolateral surface of the femoral neck; C: coronal view in T2 sequence showing exostosis of the femoral neck and signs consistent with anterosuperior labral rupture.
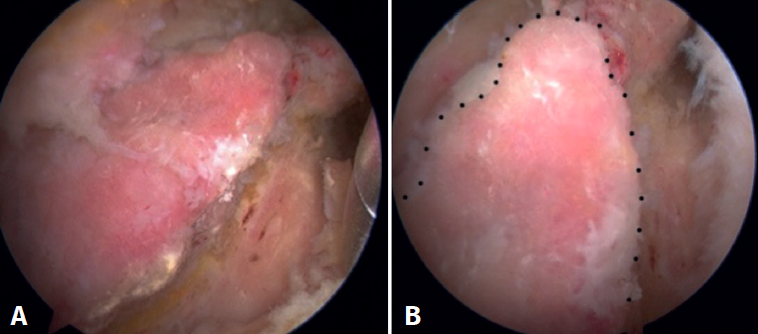
Figure 3. A: arthroscopic view of the peripheral compartment from the anterior portal, showing the tumour of the femoral neck; B: arthroscopic view of the peripheral compartment from the anterolateral portal, showing the tumour (highlighted by a broken line) of the femoral neck.
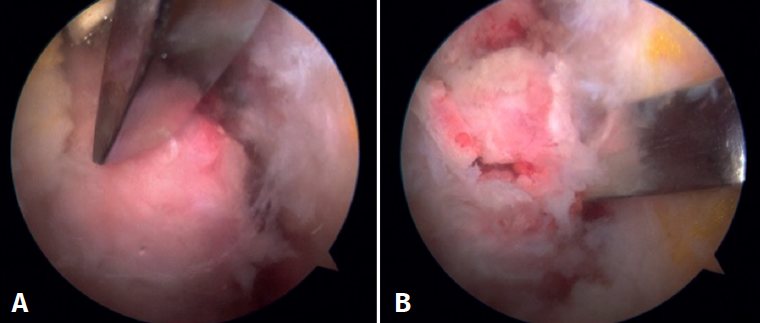
Figure 4. Arthroscopic view of the peripheral compartment from the anterior portal, corresponding to different moments of biopsy sampling with the 5-mm osteotomy.
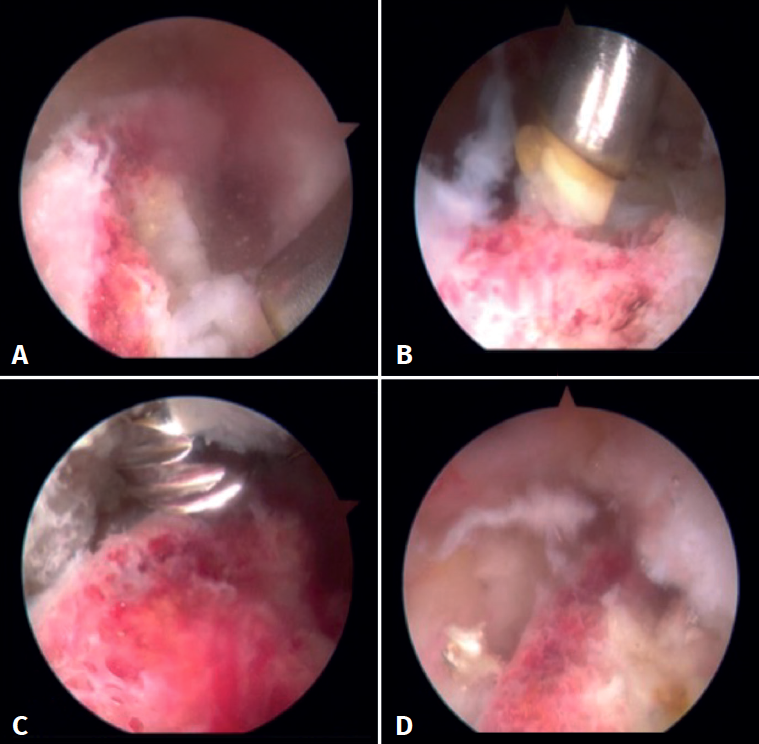
Figure 5. Arthroscopic view of the peripheral compartment from the anterior portal, corresponding to different moments of radiofrequency individualisation and tumour resection using a 4-mm round bur.
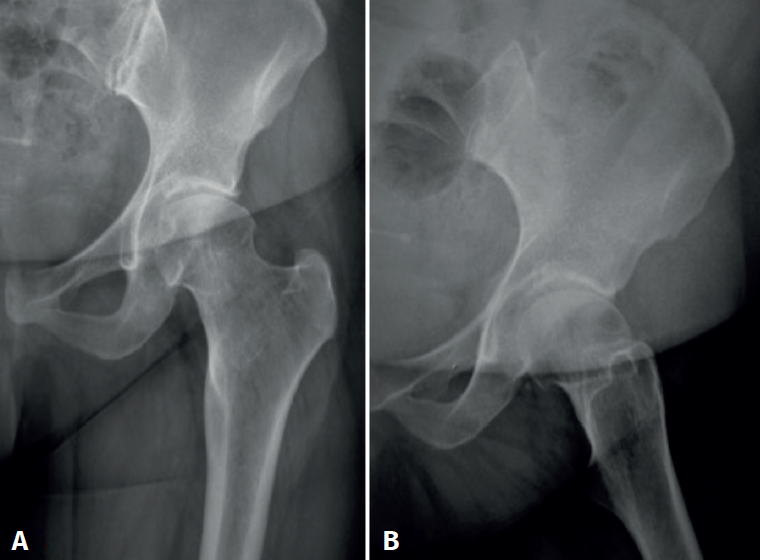
Figure 6. A: anteroposterior plain X-ray view of the left hip, following arthroscopic resection of the tumour; B: axial plain X-ray view of the left hip, following arthroscopic resection.
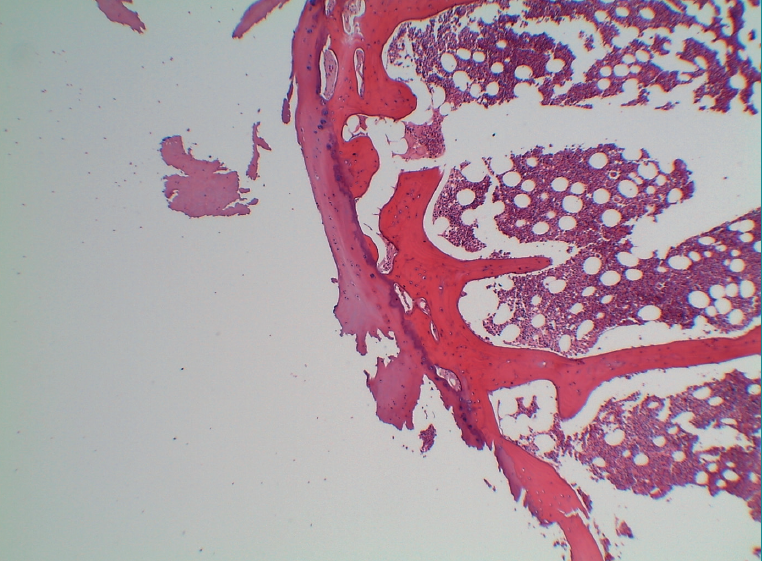
Figure 7. Histological view of the sample, showing a peripheral capsule of mature cartilage, chondrocytes with a small nucleus and vacuolated cytoplasm, no signs of atypia, and showing enchondral ossification with preserved trabeculae, in the context of signs of haemorrhage and mild chronic inflammation (HE, x4 magnification).
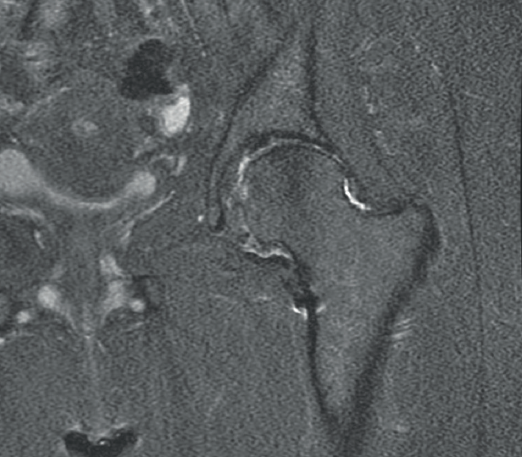
Figure 8. Coronal magnetic resonance imaging view in T2 sequence showing decreased joint cartilage and impingement of the femoroacetabular space.

Figure 9. Sample of the femoral head sent for pathology study in the arthroplasty procedure, showing the zone resected in the previous surgery and the loss of cartilage thickness in the anterosuperior zone of the head.
Información del artículo
Cita bibliográfica
Ethical responsibilities
Conflicts of interest. The authors state that they have no conflicts of interest.
Financial support. This study has received no financial support.
Protection of people and animals. The authors declare that this research has not involved human or animal experimentation.
Data confidentiality. The authors declare that the protocols of their work centre referred to the publication of patient information have been followed.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
Descargar artículo:
Licencia:
Este contenido es de acceso abierto (Open-Access) y se ha distribuido bajo los términos de la licencia Creative Commons CC BY-NC-ND (Reconocimiento-NoComercial-SinObraDerivada 4.0 Internacional) que permite usar, distribuir y reproducir en cualquier medio siempre que se citen a los autores y no se utilice para fines comerciales ni para hacer obras derivadas.
Comparte este contenido
En esta edición
- <em>REACA</em>, the journal of everyone
- Applicability of consensus methods in hip arthroscopy: a systematic review
- Evolution of the indication of arthroscopic treatment for femoroacetabular impingement and of the indication of total hip arthroplasty in patients under 60 years of age
- Evolution of glenohumeral bone defects following failed arthroscopic Bankart repair. Study of a case series
- Important articles for the surgical treatment of lateral ankle instability
- Posterolateral elbow instability with osteochondral defect of the <em>capitellum</em>; how to deal with this combination?
- Arthroscopic treatment of a femoral osteochondroma as a cause of femoroacetabular impingement. A case report
- Arthrofibrosis in the mirror
Más en PUBMED
Más en Google Scholar
Más en ORCID

Revista Española de Artroscopia y Cirugía Articular está distribuida bajo una licencia de Creative Commons Reconocimiento-NoComercial-SinObraDerivada 4.0 Internacional.