
Partial ruptures of the rotator cuff
Roturas parciales del manguito rotador
Introduction
Rotator cuff lesions are one of the main reasons for consultation in shoulder disorders. These injuries are difficult to classify and interpret, since with the exception of those few cases in which there is a clear history of trauma, they are typically progressively degenerative soft tissue disorders that only produce bone alterations in the final stages. Partial ruptures of the rotator cuff (PRRC) are set within the "grey zone" of transition between healthy tendons and full thickness ruptures. Furthermore, radiological lesions are not always pathological(1), and this further complicates their study and management. Due to the above and the limited available literature compared with full or complete ruptures, there is still much controversy in this field. A good approach to this disorder could be afforded by the recent review article published by the American Academy of Orthopedic Surgeons (AAOS)(2).
The aim of this study is to review studies of importance in view of their impact or methodology that allow us to understand the anatomy and function of the posterosuperior cuff, the natural history of the disorder and its correlation to the clinical manifestations, as well as the main treatment options for adequately diagnosing and treating our patients.
Understanding the anatomy: Clark et al. (1992)(3)
In this exhaustive anatomical study entitled: “Tendons, ligaments and capsule of the rotator cuff. Gross and microscopic anatomy”, published in 1992, Clark and Harryman offer a detailed gross and microscopic description of the rotator cuff. These authors studied 32 healthy rotator cuffs in cadavers and established their histological configuration in the form of layers, with a description of how these in turn interlink to form other structures.
This study established the bases of the 5 histological layers of the tendon-capsule complex that remain in force today. From surface to in depth, these layers are arranged as follows: the most superficial layer contains arterioles and lies in continuity with the coracohumeral ligament (CHL). Beneath this layer we find thick fibrous and organized bundles, while the third layer is characterized by fine and disordered bundles. The fourth layer is composed of lax connective tissue and thick collagen bundles that merge with the CHL at the most anterior margin of the supraspinatus muscle, while the last layer, in relation to the joint, is composed of the glenohumeral capsule and the Sharpey fibers, forming the interface with the bone.
At gross or macroscopic level, the authors found the supraspinatus (SE) and infraspinatus (IE) to merge 1.5 cm before their insertion in the bone. From the posterior zone, this common insertion is joined by the teres minor (Rm), while anteriorly, through the top and bottom of the groove, it inter-crosses with the subscapularis (SbE). This study already described a visible thickening on the capsular side in the form of a cable-like structure, to which Burkhart would give functional meaning.
Anatomy is function: Burkhart et al. (1993)(4)
This study, entitled: “The rotator crescent and rotator cable: An anatomic description of the shoulder's "suspension bridge"”, published just one year later, added a key functional anatomical concept in the operating mechanism of the rotator cuff, known as the "rotator cable". As early as 1931, Codman and Akerson described the "critical zone" where most cuff ruptures begin(5). Burkhart, as an arthroscopist, noted that this weaker crescent-shaped zone was surrounded by a thickening of the capsule, as had been described by Clark et al.(3). After dissecting 20 cadavers and obtaining measurements of the thickness of the tissue, he found that the mentioned cable has 2.55 times the thickness of the crescent on average, and moreover, in elderly shoulders, the cable appears to thicken further as an adaptive response. In this way, Burkhart described the anatomical structure that intervenes in the functioning of his biomechanical model of the posterosuperior cuff(6): the rotator cable acts as a suspension bridge in its transmission of tension forces, with an anterior anchoring post that extends from the anterior region of the SE to 40% of the IE. In this way, the cuff continues to function despite ruptures that appear with advancing age in the crescent zone (Figure 1).
reacae.30380.fs2310027en-figure1.png

Figure 1. Schematic representation of the functioning of the rotator cable suspension system. GT: greater trochanter; LT: lesser trochanter; RC: rotator cable. * "Crescent" zone.
Not everything is tendon; the importance of the capsule: Nimura et al.(7) (2012)
Historically, cuff surgery has focused on repair of the insertion of the tendon. However, over the last decade there has been a strong rise in interest in the study of the capsule and the role it plays in the biomechanics of the shoulder, to the point where the two structures are now considered to be complementary and necessary for conforming the capsule-tendon complex(8). Although the anteroinferior capsule is well known for its role in glenohumeral instability(9), the posterosuperior capsule has long drawn little attention. At present, it is accepted that the superior capsule plays a fundamental biomechanical role in glenohumeral stability, since it acts as a fulcrum and prevents upper escape of the humerus(10). The current importance of the capsule is great - to the point where in the event of non-repairable massive rotator cuff ruptures, superior capsular reconstruction (SCR) techniques have been developed involving different types of grafts. The initial results are promising, though their long term role remains to be clarified(11,12).
Nimura et al. carried out a nice anatomical study entitled: “The superior capsule of the shoulder joint complements the insertion of the rotator cuff”. After dissecting the layer composed only of the capsule, isolating it from the rest of the cuff, these authors found that, surprisingly, the posterosuperior capsule represents a greater than expected percentage of the footprint, and furthermore, its thickness is not uniform. In effect, while it occupies almost the entire width of the insertion at the lowermost zone of the IE (> 60%), it present a minimum thickness of approximately 20% at a distance of 11 mm from the anterior margin of the greater tuberosity. It is precisely in this region of minimum capsule thickness where most cases of PRRC begin; hence, this weak zone appears to play an important role in the etiology of cuff rupture.
Classification of ruptures: Ellman et al. (1990)(13)
In 1990, Ellman published a narrative review of PRRC. Although no longer up to date, it is historically interesting to know the role played during the early days of cuff surgery by diagnostic techniques such as arthrography, as well as the treatments such as open repair, that are less widely used nowadays. In the above mentioned review, the authors defined PRRC according to its location and extension in the thickness of the tendon, taking 12 mm to represent 100%. This gave rise to a classification based on the arthroscopic findings that remains in force today and is the most widely used system (Table 1). Snyder later developed another classification based on the arthroscopic findings, though it is more complex and thus less commonly used(14).
reacae.30380.fs2310027en-table1.png
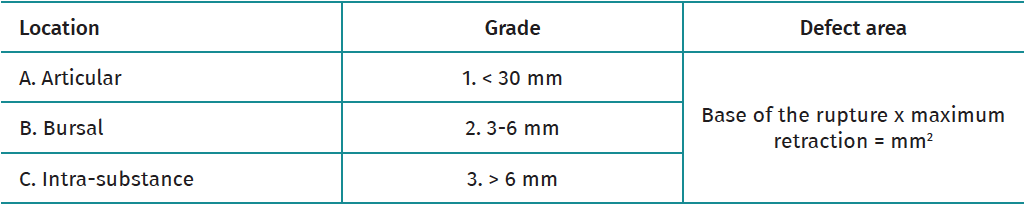
Table 1. Ellman classification of partial ruptures of the rotator cuff
Radiological prevalence of ruptures: Sher et al. (1995)(1)
In 1995, Jerry Sher and his team recruited 96 healthy volunteers with no history of shoulder or neck symptoms that were subjected to magnetic resonance imaging (MRI) study by two expert radiologists, in search of possible cuff ruptures. In addition, the MRI scans of 20 pathological shoulders were included as controls in which arthroscopy had been performed with a correct diagnosis in 100% of the cases according to the report of the radiologists. The results obtained were published in the study entitled: “Abnormal findings on magnetic resonance images of asymptomatic shoulders”.
This is a very interesting study, with a good methodological design, that provides information on the expected prevalence of asymptomatic cuff injuries and their relation to age. Although the prevalence of partial or complete ruptures is almost 0% in individuals under 40 years of age, we observe a prevalence of PRRC of 24% in the 40-59 years age interval and a 4% prevalence of full ruptures. In turn, among individuals over 60 years of age, the prevalence of PRRC reaches 26% and that of full rupture of the rotator cuff (FRRC) reaches 28%. In sum, the mentioned study shows that the cuff begins to degenerate at between 40-60 years of age, and that we must be cautious in correlating the clinical data to the radiological findings, since almost 60% of all subjects over 60 years of age who have never presented symptoms are seen to have degenerative injuries of one grade or other (Figure 2).
reacae.30380.fs2310027en-figure2.png
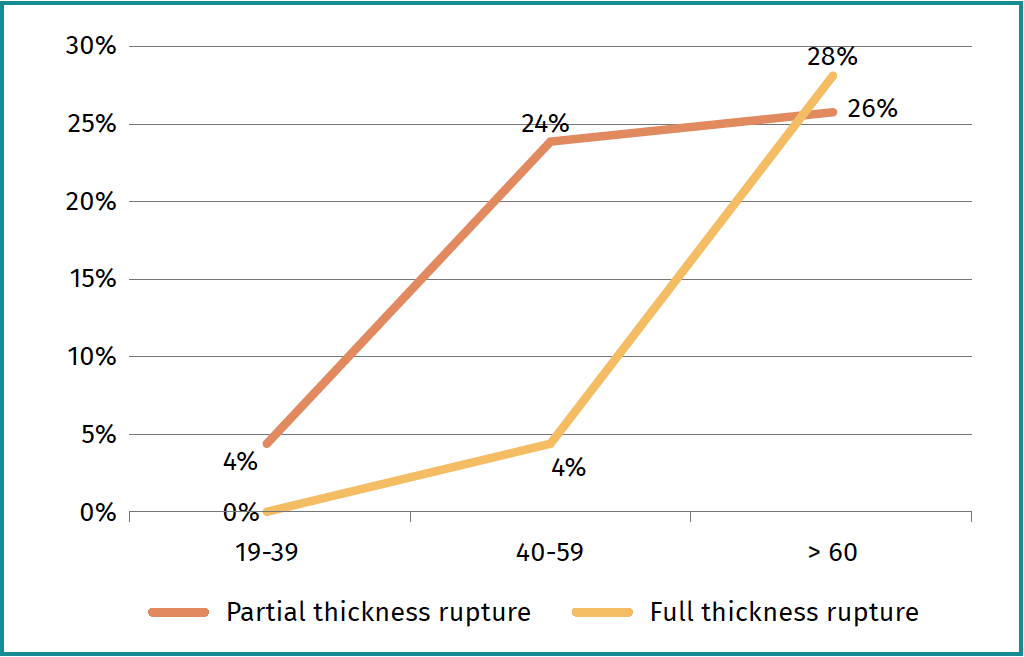
Figure 2. Prevalence of cuff ruptures in asymptomatic patients.
Natural history of the rotator cuff: Keener et al. (2015)(15)
While Sher provided information on prevalence based on a cross-sectional study of asymptomatic lesions of the cuff, Keener et al., in a prospective longitudinal study entitled: “A prospective evaluation of survivorship of asymptomatic degenerative rotator cuff tears”, described how these asymptomatic shoulders evolve based on an annual clinical and ultrasound follow-up of 118 patients divided into three groups: patients with partial rupture, patients with full rupture, and healthy controls.
Their most relevant conclusion was that the main risk factor for progression of the lesion is a greater degree of initial tear or rupture. In effect, while only 14% of the controls presented some type of rupture, 44% of the patients with PRRC and 60% of those with FRRC significantly progressed at least 5 mm. Furthermore, the appearance of pain was associated with the presence of rupture progression. The authors also found that those patients with greater rupture at the end of follow-up had initially started with symptoms in a larger percentage of cases, though 28% of the individuals without rupture also presented symptoms.
Another interesting aspect of this study is referred to the survival curves, as these explain not only the low risk of progression of PRRC, but also that when rupture progresses, it takes an average of 3.3 years in doing so. Such information indicates that this is a slow degenerative process, and allows us to study our patients and assess the treatment options without urgency. In 2023, these same authors analyzed the course of asymptomatic ruptures in a young population (< 65 years of age) over a median follow-up period of 7.1 years. Similar results were recorded in this specific population group, with a progression-free survival rate of 73% at 5 years and a median time to progression of 4.9 years. Thus, in young individuals of working age we also have sufficient time for adequate assessment and definition of a monitoring plan(16).
On combining the data of the last two studies commented above, it can be concluded that the prevalence of cuff injuries is high, particularly in individuals over 60 years of age, and that these injuries should not always be regarded as pathological. However, we need to be alert to cases of advanced lesions with the appearance of pain, since rupture may be progressing - though progression in most cases takes several years.
Controversies of surgical treatment; when to operate: Kim et al. (2018)(17)
One of the main controversies in PRRC refers to the best management strategy, since there are almost no quality studies on this issue. At present, most surgeons advise initial conservative management for at least 3-6 months, based on the clinical-radiological dissociation, the low probability of progression and - in those cases that do progress - the time needed for actual progression to take place(18). The aim of conservative management is to keep the shoulder functional without pain, or with tolerable pain, since it is known that the tendon is unable to spontaneously repair itself without surgery(19). This aim is sometimes not reached, however, and the possibility of surgery is then considered.
In view of the concern of some surgeons that partial rupture may progress quickly to the point of losing the time window for repair, the authors of the clinical trial entitled: “When should we repair partial-thickness rotator cuff tears? Outcome comparison between immediate surgical repair versus delayed repair after a 6-month period of nonsurgical treatment” compared the results of immediate surgery versus delayed surgery after 6 months of conservative management in patients who had experienced symptoms for less than three months. The investigators found that 6 months after surgery, those patients who had received conservative management preoperatively had better clinical outcomes, though after 12 and 24 months of postsurgical follow-up the clinical outcomes became equalized, with the same healing rate in the MRI control study. In addition, of the 44 patients in the delayed treatment arm, 10 abandoned the study voluntarily due to improvement of the symptoms. Thus, it seems very reasonable to offer at least 6 months of conservative management in cases of symptomatic PRRC, since there is a possibility of improvement without compromising the outcomes of potential surgery.
Randomized prospective trials of this kind contribute quality data for establishing therapeutic recommendations, though methodologically well designed studies are needed to adequately define the different conservative treatment options and their long term outcomes.
Repair versus conversion: Shin (2012)(20).
As mentioned, it is commonly accepted to offer surgical repair in symptomatic patients after a period of at least 6 months of conservative management and with involvement of over 50% of the cuff thickness(2). The two most common techniques in joint ruptures are in situ trans-tendon repair (debridement of the torn tendon and suturing in which there is contact between the latter and the bone, keeping the remnant in continuity with the footprint) and conversion and repair (completion of the rupture followed by suturing as in FRRC). However, while completion of the tear guarantees removal of the degenerated tissue and suturing with viable tissue, the fact that the remnant is sacrificed causes concern with regard to healing after full rupture. In the study entitled: “A comparison of two repair techniques for partial-thickness articular-sided rotator cuff tears”, Shin randomized 48 patients to one or the other repair technique, with follow-up over two years. Clinically, although the patients subjected to conversion and repair were better after three months, the outcomes were seen to be equivalent over the rest of follow-up. The repair group showed a high repeat rupture rate (0% versus 8%), though the patient outcomes were not worsened as a result. Other later studies likewise have reported no differences between the two techniques; as a result, it is currently not possible to recommend one option in preference to the other(21,22).
Conclusions
The mentioned studies define the histology and gross anatomy of the posterosuperior cuff. In the biomechanics and pathology of partial ruptures, it is important to note that there is a weak zone at the posterior limit of the SE, and to understand how the "rotator cable" capsular thickening works to transmit force when rupture begins. The appearance of PRRC starts in the fifth decade of life and increases with age, though several years are needed for progression to take place. The first therapeutic option in PRRC is conservative management for at least 6 months, though the best conservative protocol has not been established to date. In those cases where surgery is required, the results of "in situ" repair versus conversion and repair are equivalent. The surgeon therefore must choose the best strategy according to the patient involved and his or her personal experience.
Figuras
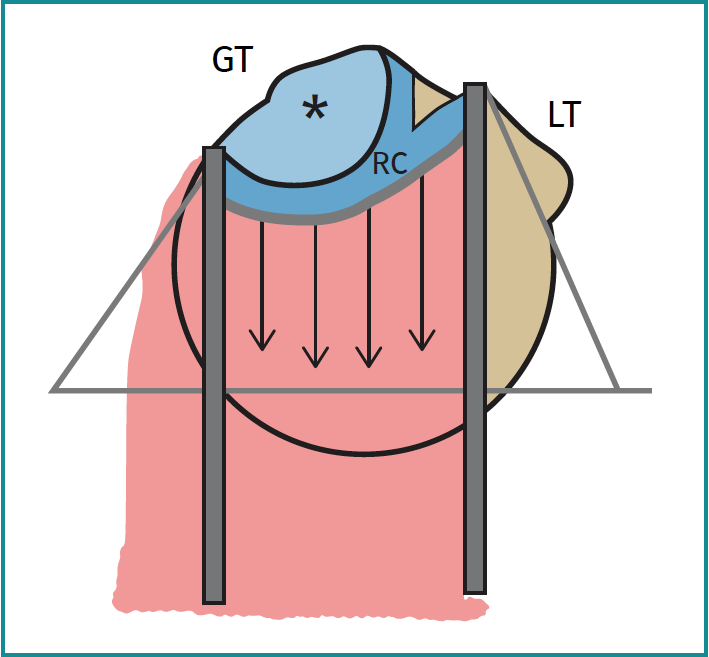
Figure 1. Schematic representation of the functioning of the rotator cable suspension system. GT: greater trochanter; LT: lesser trochanter; RC: rotator cable. * "Crescent" zone.
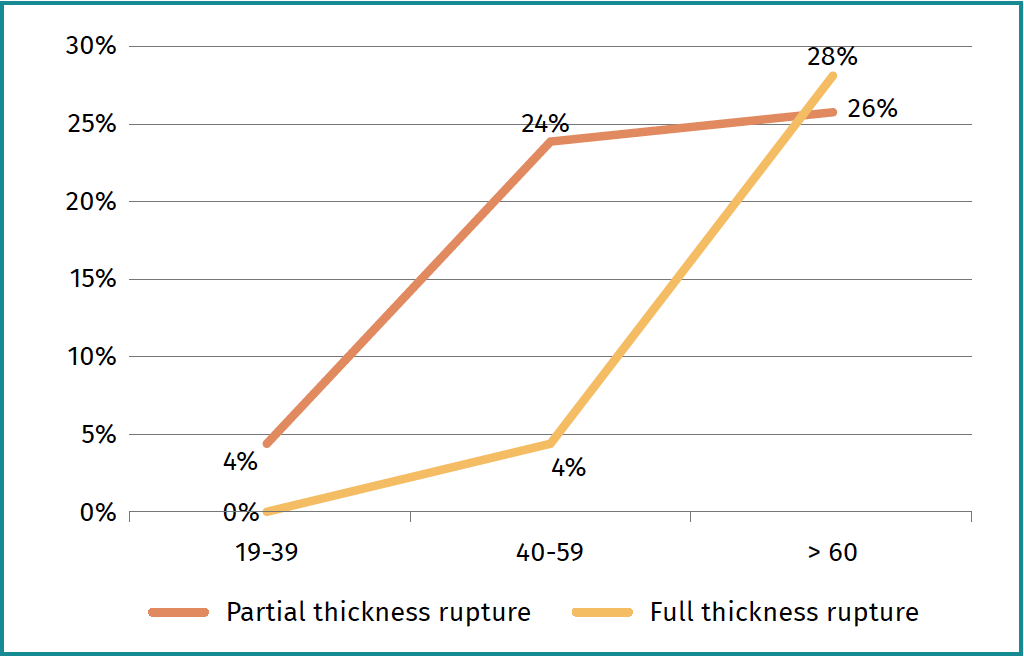
Figure 2. Prevalence of cuff ruptures in asymptomatic patients.
Tablas
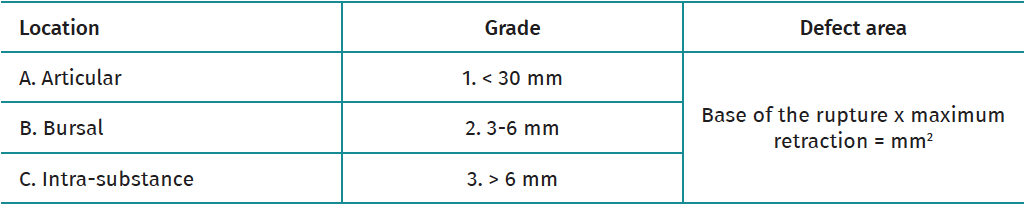
Table 1. Ellman classification of partial ruptures of the rotator cuff
Información del artículo
Cita bibliográfica
Ethical responsibilities
Conflicts of interest. The authors state that they have no conflicts of interest.
Financial support. This study has received no financial support.
Protection of people and animals. The authors declare that this research has not involved human or animal experimentation.
Data confidentiality. The authors declare that the protocols of their work centre referred to the publication of patient information have been followed.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
Descargar artículo:
Licencia:
Este contenido es de acceso abierto (Open-Access) y se ha distribuido bajo los términos de la licencia Creative Commons CC BY-NC-ND (Reconocimiento-NoComercial-SinObraDerivada 4.0 Internacional) que permite usar, distribuir y reproducir en cualquier medio siempre que se citen a los autores y no se utilice para fines comerciales ni para hacer obras derivadas.
Comparte este contenido
En esta edición
- From the start to the top: the history of knee osteotomies
- Clinical-functional and radiographic outcomes of medial valgus-producing tibial osteotomy
- Patellar tendinopathy: a practical consensus guide for choosing the best treatment
- Evolution of spinal endoscopy. Where do we come from and where are we going?
- Partial ruptures of the rotator cuff
- Arthroscopic core decompression of the femoral head with autologous stem cell placement as treatment for femoral head osteonecrosis
- Extraarticular plasty as sole maneuver in the correction of rotational instability due to rupture of the anterior cruciate ligament in an elderly patient
- Fully arthroscopic osteosynthesis with button placement in acute anterior glenoid fracture: a case report
- Arthroscopic visualization of the popliteal hiatus and localization of an intraarticular free body
Más en PUBMED
Más en Google Scholar
Más en ORCID

Revista Española de Artroscopia y Cirugía Articular está distribuida bajo una licencia de Creative Commons Reconocimiento-NoComercial-SinObraDerivada 4.0 Internacional.