
Patellar tendinopathy: a practical consensus guide for choosing the best treatment
Tendinopatía rotuliana: una guía práctica de consenso para la elección del mejor tratamiento
Introduction
Patellar tendinopathy is characterized by anterior knee pain fundamentally located in the lower pole of the patella(1), in the deep portion of the tendon. It accounts for 30-45% of all lesions experienced by jumping athletes, causing inactivity periods of as long as 6 months(2). Conservative management constitutes the first line treatment option. When conservative management fails, open, arthroscopic and ultrasound-guided surgery have been described(3) for the treatment of these disorders, with variable techniques and consistent outcomes(4).
However, the literature describes treatment options with different mechanisms of action and degrees of effectiveness that complicate decision making in daily clinical practice(5,6).
The present study describes the most common treatment options, detailing the level of evidence for their application, and finally offers a grade of recommendation for each of them, from the Muscle and Tendon Injuries Working Group (Grupo de Estudio de Lesiones Músculo Tendinosas [GELMUT]) of the Spanish Association of Arthroscopy (Asociación Española de Artroscopia [AEA])(Table 1).
reacae.30380.fs2211023en-table1.png
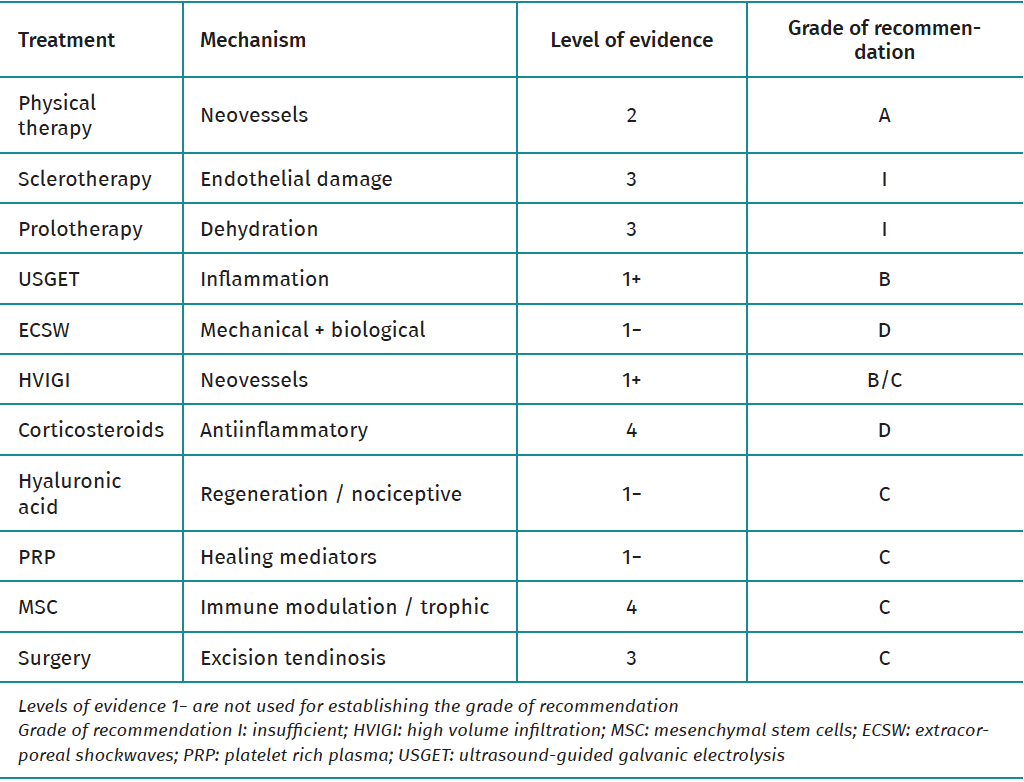
Table 1. Treatment alternatives in patellar tendinopathy.
For this purpose, a narrative review of the scientific literature has been made, involving a search of the PubMed and Cochrane databases using the keywords "patellar tendinopathy treatment". The citation of an article required it to meet the following criteria: an original paper, in English / Spanish, with description of the results of the intervention based on a validated scale and/or the contribution of data of historical value for understanding of the therapeutic technique. On the other hand, in order to establish the recommendations, selection was made of articles with a Jadad score of > 3(7), and the scale suggested by The Journal of Bone and Joint Surgery (JBJS)(8) was used to generate the grades of recommendation. This scale establishes grade A for recommendations based on consistent level I studies that generate good evidence in favor or against a given intervention; grade B for recommendations based on level II or III studies that generate sufficient evidence in favor or against; grade C when the available evidence is conflictive or of poor quality, based on level IV or V studies; and grade I when there is not enough evidence to offer a grade of recommendation.
Physical therapy
Physical therapy constitutes the first line treatment option for tendinopathy(9). In this context, protocols involving eccentric loading exercises, initially described by Stanish et al.(10), are the most widely used strategy.
It has been postulated the eccentric exercises could induce metabolic changes in the tendon by interrupting neovascular blood flow, and thus lead to clinical improvement. However, within dynamic loading, no differences in cellular changes are observed between healthy tenocytes subjected to concentric or eccentric loading(11).
In 2011, Larsson et al. published a systematic review of randomized clinical trials, postulating that there is firm evidence in support of the use of eccentric exercises in the treatment of patellar tendinopathy(12), since statistically significant differences were recorded in 5 of the 7 articles considered to be of high quality, comparing the effectiveness of eccentric treatment versus another treatment modality. However, due to the variability of the clinical trial protocols, no single protocol can be recommended - though it has been suggested that the combination with stretch exercises affords better results than eccentric exercises alone(13).
Conclusions and grade of recommendation
Eccentric exercises should be the cornerstone of treatment in patellar tendinopathy. There is strong evidence in favor of the use of such exercises. Stretch and progressive strength exercises combined with eccentric loading could offer greater benefit versus eccentric exercises alone.
Grade of recommendation: A.
Sclerotherapy and prolotherapy
Sclerotherapy intends to produce a sclerotizing effect upon the nociceptive nerve endings associated with tendinopathy(14), and on the neovessels that form in hypervascular tendinopathies. Polydocanol, a topical anesthetic that causes endothelial damage on interacting with the lipid layer of the cell membrane, is usually used for this purpose. There are no randomized studies demonstrating its efficacy(15). Furthermore, attributing pain in tendinopathy to the appearance of neovessels is currently subject to controversy(16,17).
On the other hand, prolotherapy involves the injection of hyperosmolar substances, generally dextrose(17), that attract macrophages and granulocytes on damaging the cells through dehydration. The appearance of these cells could favor healing, though the underlying mechanism of action is not fully clear(18,19).
Conclusions and grade of recommendation
At present there are not enough studies on sclerotherapy and prolotherapy demonstrating clinical improvement in the treatment of patellar tendinopathy. Their use therefore cannot be recommended.
Grade of recommendation: I.
Ultrasound-guided galvanic electrolysis (USGET)
Ultrasound-guided galvanic electrolysis (USGET) involves the application of a non-thermal galvanic current under ultrasound guidance to induce a controlled local inflammatory reaction. It has been reported that the application of electrical fields is associated with elevated collagen synthesis and an increase in intracellular Ca++(20).
Abat et al.(21) showed that the combination of USGET with eccentric exercises in the treatment of patellar tendinopathy in 41 patients yielded good outcomes, without recurrences after 10 years of follow-up. In 2016, the same authors published a clinical trial22 in which 60 patients with patellar tendinopathy were divided into two groups. The first group underwent physiotherapy with ultrasound, laser and interferential currents. The second group was subjected to USGET therapy. The Victorian Institute of Sports Assessment for Patellar Tendinopathy (VISA-P) evidenced improvements in both groups, though with statistically significant better outcomes in the USGET group.
López-Royo et al.(23) postulated that there are no clinically significant differences when treatment is based on an eccentric exercises program (combined or not with electrolysis or dry needling), though their follow-up period was limited to only 22 weeks.
Conclusions and grade of recommendation
The current evidence warrants the use of USGET in patellar tendinopathy, combined with an eccentric exercises program. It is necessary to protocolize the indication and the methodology (in terms of intensity and the number and frequency of sessions), as well as to demonstrate its superiority versus other techniques that stimulate tissue repair.
Grade of recommendation: B.
Shockwave therapy
Shockwave therapy has been used in tendinopathies since the 1990s(24). It has been postulated that this type of treatment exerts an analgesic and regenerative effect upon the tendon, with the observation of an increase in collagen synthesis in animal models(25). Shockwaves are able to exert a combination of mechanical effects (through the destruction of cells and membranes) and biological actions (increasing the synthesis of proteins involved in the tissue repair process)(26). They have been found to offer some effectiveness in treating plantar fasciitis and calcific tendinopathy of the rotator cuff(27).
A number of randomized clinical trials have compared shockwave therapy with other treatment alternatives in the management of patellar tendinopathy. These studies have obtained heterogeneous results(28,29,30,31,32). In this respect, in 2003, Peers et al.(28) studied 27 patients in which shockwave therapy was compared against surgery, with the observation of similar functional outcomes after 6 months of follow-up. In 2011, Zwerver et al.(29)compared effectiveness in 62 athletes during the competition season, and recorded no differences between the two groups.
Vetrano et al.(30), in 2013, administered shockwaves to 23 patients, with the injection of autologous platelet rich plasma (PRP) in a second group of 23 subjects. Both groups showed improvement, though to a greater extent in the PRP group. In 2017, Thijs et al.(31) carried out a clinical trial comparing shockwaves versus placebo in 52 patients, and recorded no statistically significant differences between the two groups. The main weakness of this study was the dropout rate during the 24 weeks of follow-up.
In 2018, Cheng et al.(32) conducted a clinical trial comparing shockwave therapy (n = 26) versus physical therapy (n = 25), with the inclusion in the latter group of microwaves, acupuncture and ultrasound. Improvement was found to be significantly greater in the shockwave therapy group.
Conclusions and grade of recommendation
The current evidence on the treatment of patellar tendinopathy using shockwaves is based on heterogeneous studies, with diverse control groups and a generally limited number of patients. The studies present low evidence of good outcomes in treating chronic patellar tendinopathy; shockwave therapy therefore cannot be recommended.
Grade of recommendation: C.
Infiltrations
Treatment in the form of infiltrations is one of the most widely used strategies in the conservative management of patellar tendinopathy. There is controversy as to whether infiltration should be made in the tissue lesion zone or in the surrounding area. The injections must be guided by real-time ultrasound or anatomical reference points(33). Different types of injections can be used, as detailed below.
High volume
High volume image-guided injection (HVIGI) targets neovascularization visualized by doppler ultrasound. A combination of local anesthetic and saline solution is usually employed.
The mechanism of action of HVIGI is explained by the mechanical aggression (stripping) of the fluid upon the neovascularization, stretching, rupturing or occluding the neovessels and the accompanying nerve supply(34), along with the possible toxicity of the local anesthetic through the reduction of substance P - a known neurotransmitter involved in the increased inflammatory and nociceptive response in the nerve fibers(35,36).
The technique consists of the ultrasound-guided injection of saline solution and a local anesthetic (bupivacaine or mepivacaine) into the space between the patellar tendon and its sheath, at posterior level(37). The injected volume should exceed 50 ml (with only 20% corresponding to the anesthetic), since the results have been shown to be better than when administering less than 30 ml(38). No major complications have been reported with this procedure(39).
Maffulli et al.(40) evaluated the efficacy of high volume injections in 32 patients with patellar tendinopathy. Seventy-two percent of the patients returned to the same level of activity as before the symptoms, and 80% described their condition as good or excellent. Posteriorly, the clinical outcomes were seen to improve with the simultaneous administration of PRP(41). Morton et al.(34) obtained similar results in a combined retrospective and prospective series of cases.
Recently, Barker-Davies et al.(37), in a randomized, double-blind, controlled clinical trial, recorded no significant differences between the use of HVIGI, local anesthetic without high volume, and HVIGI with corticosteroids, after 6 months of follow-up in a military population. At the end of this period, the three treatment groups showed improved pain (visual analogue scale [VAS]) and function scores (VISA-P) versus the pre-treatment phase, with no differences among the groups. Likewise, the authors recorded no differences in the thickness of the tendon or in its neovascularization after 6 months of follow-up.
Corticosteroids
Although it is currently accepted that inflammation is not the fundamental cause of tendinopathies, the use of corticosteroids in these disorders remains a common practice. In addition to their known potent antiinflammatory action (which could play a role in the acute phase of the injury), corticosteroids affect the synthesis of extracellular matrix, the production and depositing of collagen, scar formation and tenocyte proliferation and viability, inducing cell death, tendon atrophy and favoring the formation of adherences between the tendon and the surrounding tissues(42,43). On the other hand, they exert a vasoconstrictor effect upon the smooth muscle cells, resulting in a decrease in nitric oxide production and, possibly, a decrease in pain. Thus, corticosteroids appear to offer pain relief over the short term, though there is little evidence on their long term benefits(43,44,45).
Most authors advise infiltration in the posterior peritendinous zone, due to the risk of damaging the tendon, or at the interface between Hoffa's fat pad and the patellar tendon, with the knee in full extension or slight flexion in order to expose the tendon from the medial side of the knee.
Kongsgaard et al.(46) compared the efficacy of methylprednisolone injection, eccentric exercises and slow resistance training in patellar tendinopathy. The results evidenced an immediate improvement of the pain and VISA-P score with all the treatment methods, though a worsening of the VISA-P score was noted at 6 months in the injection group. In 2017, Everhart et al.(47) carried out a systematic review of the treatment options in patellar tendinopathy, and concluded that corticosteroid injections should not be used to treat this disorder, since no benefits were observed with their use(48).
Hyaluronic acid
Hyaluronic acid (HA) is one of the main components of synovial fluid and the tendinous extracellular matrix, and can be produced in the normal tendon sheath. In vitro and nonclinical studies have shown HA to offer useful properties for tendon healing. In addition, in clinical studies, HA has been used with promising results in tendinopathies of different locations such as the shoulder, elbow, knee and ankle(49). High molecular weight HA has inflammatory properties and can promote tissue regeneration and favor healing of the tendon at the bone-tendon interface(50). It has also been suggested to reduce nociceptive nerve activity(51).
The treatment is administered as an ultrasound-guided injection, in the same way as described in the case of corticosteroids. However, the literature is variable in terms of the number and periodicity of the injections(52,53). Allergic reactions have been reported as possible complications(39).
Different series describe good outcomes in terms of pain relief over the short term(52,54,55). On the other hand, Kaux et al.(53), in a clinical trial, compared ultrasound-guided injections of PRP versus two injections of HA, and found that both treatments may be effective: the PRP group showed significant improvement of quadriceps strength, while HA had a greater impact in terms of symptoms improvement. Recently, Frizziero and his team(56) reported good results after three injections of HA of medium molecular weight guided by ultrasound. This study reported pain relief and improvement of the VISA-P scores after 90 days of follow-up, with a decrease in vascularization and thickness of the tendon in the ultrasound and doppler ultrasound studies.
Platelet rich plasma
Platelet rich plasma is a fraction of autologous blood with a high content of platelets and associated growth factors that are injected at the site of muscle or tendon damage as a coadjuvant to the natural healing process.
The rationale underlying the use of PRP is that platelets are the first to reach the tissue injury site and thus have the potential to release growth factors (PDGF, TGF-β, FGF, etc.) that play a key role in the mediation of the three healing phases: inflammation, proliferation and remodeling(57). This matrix acts as a scaffold for the sustained release of growth factors that promote chemotaxis and angiogenesis(58).
In general, the preparation of PRP involves the obtainment of autologous peripheral venous blood that is centrifuged in one or two steps to separate the plasma from the red cells and leukocytes(59), though there is variability in the form of preparation and in the concentration of the platelets and leukocytes(59,60). Although the latter are important for wound healing and for facilitating tissue repair, they could induce an undesired inflammatory response at the injection site. Formulations rich and poor in leukocytes are therefore available. There is not enough in vivo evidence to suggest which preparation method is best. However, it is important to understand that there are a number of methods for obtaining and preparing PRP(59).
A number of studies have been made (summarized in Table 2) on the injection of PRP as treatment for patellar tendinopathies, comparing its efficacy versus other therapies, in terms of pain relief and functional improvement. Several of these studies(30,41,53) even report contradictory results in terms of pain relief and tissue healing properties(57,61).
reacae.30380.fs2211023en-table2.png
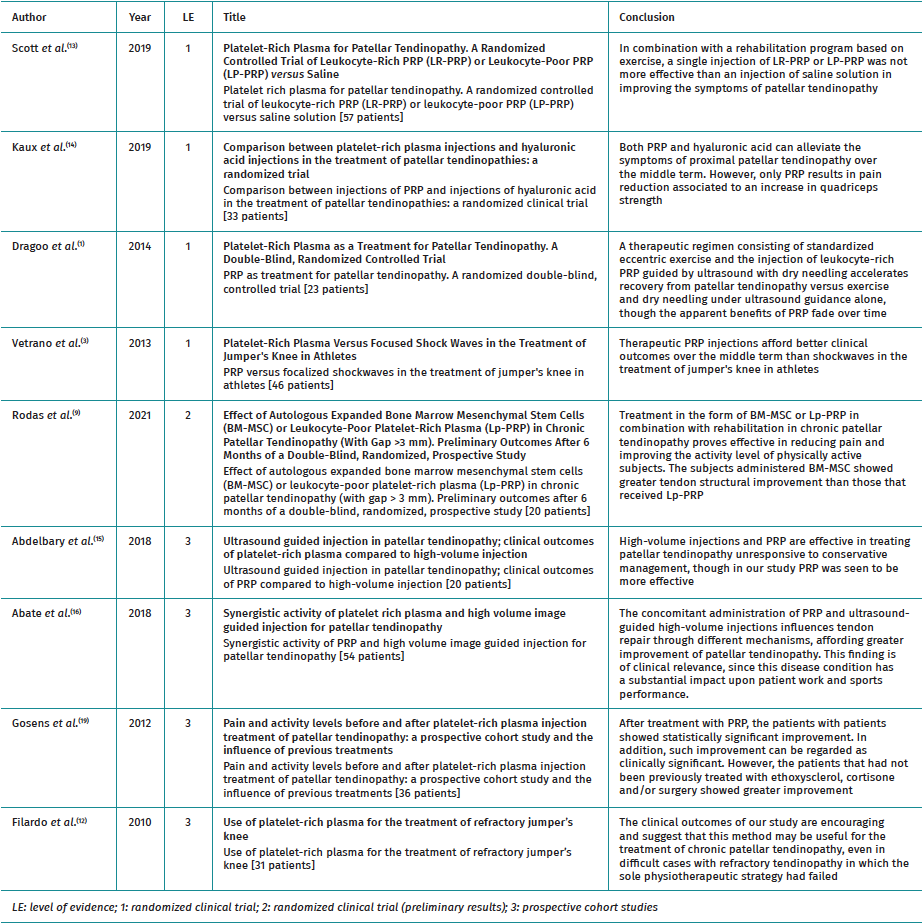
Table 2. Clinical trials and prospective cohort studies on the use of platelet rich plasma (PRP) in patellar tendinopathy.
In a recent systematic review and meta-analysis of this subject, Barman et al.(62) concluded that in terms of pain relief and the functional outcomes, the injection of PRP does not afford significantly greater clinical benefit than injections without PRP in the management of patellar tendinopathy. Nevertheless, compared with shockwave therapy, a significant benefit was indeed observed in favor of PRP injections. On the other hand, Andriolo et al.(63), likewise in a systematic review and meta-analysis, concluded that eccentric exercises may be regarded as the strategy of choice over the short term, but that PRP injections can offer better and more stable outcomes over the long term, and thus may be regarded as an adequate choice for the treatment of patellar tendinopathy.
Mesenchymal stem cells (MSC)
Mesenchymal stem cells (MSC) have shown promising results in cardiac, neurological, autoimmune and musculoskeletal disorders. They can be obtained from bone marrow (the most widely studied and used source) or from the subcutaneous adipose tissue. Although in the past attention focused on their differentiation capacity and direct participation in the regeneration process, it has recently been shown that MSC have other and probably more important therapeutic functions in response to injuries, such as immune modulation and trophic activities(5).
Some authors have published case series on the treatment of tendinopathies using MSC(64). Preclinical studies of Achilles tendinopathy in animal models have reported significant benefits with the use of autologous MSC(64,65,66). However, many issues related to the use of MSC have not been fully addressed, such as the timing of administration of the cells at the lesion site. Some studies appear to suggest that MSC should not be administered in the first phases of the lesion process, as this could result in undesired proinflammatory effects. In contrast, later injection could induce a desired immune suppression process leading to resolution of the lesion(5).
Rodas et al.(64) recently published the first clinical study in humans on the effect of MSC in application to patellar tendinopathy. Based on their preliminary results, these authors concluded that the treatment appeared to reduce pain and improve the levels of physical activity.
Conclusions and grades of recommendation
The available evidence on infiltration treatment has important limitations, such as the few high level studies and the heterogeneity of the treatment strategies and forms of application. Studies with greater methodological rigor and larger sample sizes are needed, describing the indications and protocolized methodology of use, as well as comparing the different available treatments.
The literature suggests that high volume, HA and PRP injections may be regarded as a safe option for patients with severe symptoms or when noninvasive rehabilitation strategies prove unsuccessful in treating chronic patellar tendinopathy. On the other hand, we do consider that there is enough evidence not to recommend corticosteroid injections for the treatment of patellar tendinopathy, in view of the associated complications.
Lastly, in relation to MSC in patellar tendinopathy, there is still not enough evidence to establish a recommendation.
Grades of recommendation:
- High volume, hyaluronic acid and PRP: C.
- Corticosteroids: B against their use.
- MSC: I.
Surgery
The surgical option should be offered after a guided and continued physiotherapy program lasting at least 12 weeks that should be followed by other nonsurgical treatments during the next 3-5 months, since it has been estimated that only 10% of all patients fail to respond to conservative management. Nevertheless, there are studies that postulate that the chances for successful surgical treatment decrease with every month of persistence of the symptoms(4,47,50,67,68,69,70).
Surgery offers a variable success rate of between 45-100%(4,47,50,69,70,71,72,73). Surgery should aim to remove the degenerative area of the tendon, usually located in its proximal and deep portion, though there have been descriptions of different isolated or combined procedures such as anterior longitudinal tenotomies (tendon shaving), perforation of the lower pole of the patella, and perforations or resection of the neovessels of the posterior aspect via arthroscopy(50,67,69,70).
During the open procedure, a midline approach is adopted from the lower pole of the patella to the tibial tuberosity. Opening with debridement of the peritendon is carried out, performing the incision longitudinal in order to access the deep portion of the tendon at its proximal insertion. The tendon is palpated in search of areas with tendon disease which are then excised with a cold scalpel, attempting to preserve the healthy fibers and Hoffa's fat pad as much as possible. As commented above, other maneuvers are usually added, seeking to create an environment favorable to the formation of healthy tendon tissue. According to different publications, peritendon repair could compromise the outcomes, and is therefore a controversial procedure(72).
The first description of the arthroscopic treatment of patellar tendinopathy was published in 1999(3). In 2006, Willberg et al.(74) proposed resection of the neovessels and neural tissue of the posterior aspect of the patellar tendon through their intraoperative direct visualization, with the help of ultrasound. These authors postulated that a more aggressive therapeutic alternative could shorten the duration of treatment and thus the symptoms of the patient. Posteriorly, Lorbach et al.(75) described the release of the deep fibers of the patellar tendon at proximal level, combined with resection of the lower pole of the patella, on the premise that these fibers are damaged through entrapment with the patella at the end of flexion. The ultrasound-guided surgical technique emulates the arthroscopic procedure, with the difference that it defines the level of resection with the synoviotome according to the thickness of the contralateral tendon, measured preoperatively (Figure 1).
reacae.30380.fs2211023en-figure1.png
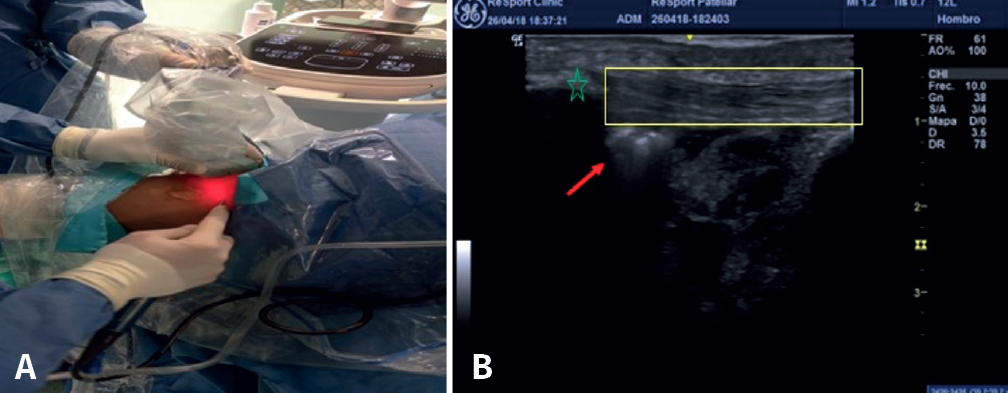
Figure 1. A: after creating the anterolateral and anteromedial knee portal 1 cm more lateral and more medial, respectively, resection is carried out of the neovessels and nerve tissue of the posterior aspect of the patellar tendon, as well as of the area of tendinosis and/or calcification in the posterior zone, until a tendon is obtained of the same thickness as the healthy contralateral tendon(74). The technique requires an assistant to hold the ultrasound device while the main surgeon controls the optics and the synoviotome. B: the red arrow indicates the location of the synoviotome over the deep zone of the patellar tendon (yellow inset). The asterisk shows the distal pole of the patella.
The patients start early physiotherapy, with free range of motion and loading, which includes the management of pain, the start of eccentric squatting on an inclined ramp(9), and a strengthening program. A return to sports activity is allowed once at least three months of supervised rehabilitation have been completed and the strengthening exercises can be performed without pain.
Surgery of patellar tendinopathy includes different techniques. It is therefore difficult to compare the results of the published studies, in the form of case series, and which in general report improvement of pain and function, with a high percentage of patients able to return to their pre-injury level of sports, and with no reported major complications(4,12,47,67,68).
In 2000, Coleman et al.(70) published a systematic review of 25 surgical treatment studies, evaluating their quality using a customized methodological scoring system. They found that in general, the quality of the studies was low. At that time there were only two prospective studies, both with a non-randomized design. Curiously, they also found the reported success rate to be inversely related to the methodological quality of the studies.
In the most recently published review (Cochrane) in 2019(76), it was considered that only a randomized study of open surgery could offer quality evidence. The conclusions that open surgery improves patient pain, function and return to activity were regarded as recommendations based on low level evidence. In turn, the conclusion referred to the absence of adverse effects in surgery was considered to be of very low certainty. The authors considered that the indication of open surgery in patellar tendinopathy is based more on the exhaustion of other therapeutic options than on the evidence of benefit of surgery. The theoretical advantages which the arthroscopic technique could offer are extrapolated from data obtained by a study with important methodological shortcomings, such as the lack of a control group, a short duration of follow-up (only 6 months), and no contrasting of hypotheses between the pre- and postoperative results(74).
Conclusions and grade of recommendation
Considering all the above, it can be affirmed that surgery appears as an aggressive solution in the face of a lack of clinical improvement following conservative management. However, the studies that endorse surgical treatment are case series that do not offer evidence of sufficient quality to establish any recommendations. In fact, the only published randomized study showed no superiority of the results versus eccentric exercise at one year of follow-up. It therefore seems logical to reserve this option for concrete cases and try to minimize surgical aggression.
Grade of recommendation: C.
General conclusions
The conservative management of patellar tendinopathy based on physical therapy in a program of supervised eccentric exercises and stretching should be regarded as the cornerstone of treatment. In addition to the above, patients can be offered invasive techniques that induce molecular changes in the tendon, such as USGET and/or infiltrations of PRP. The use of corticosteroid infiltrations is not advised. Surgery lacks robust evidence to recommend its use, and therefore should be reserved for selected cases in which conservative management has failed.
Tablas
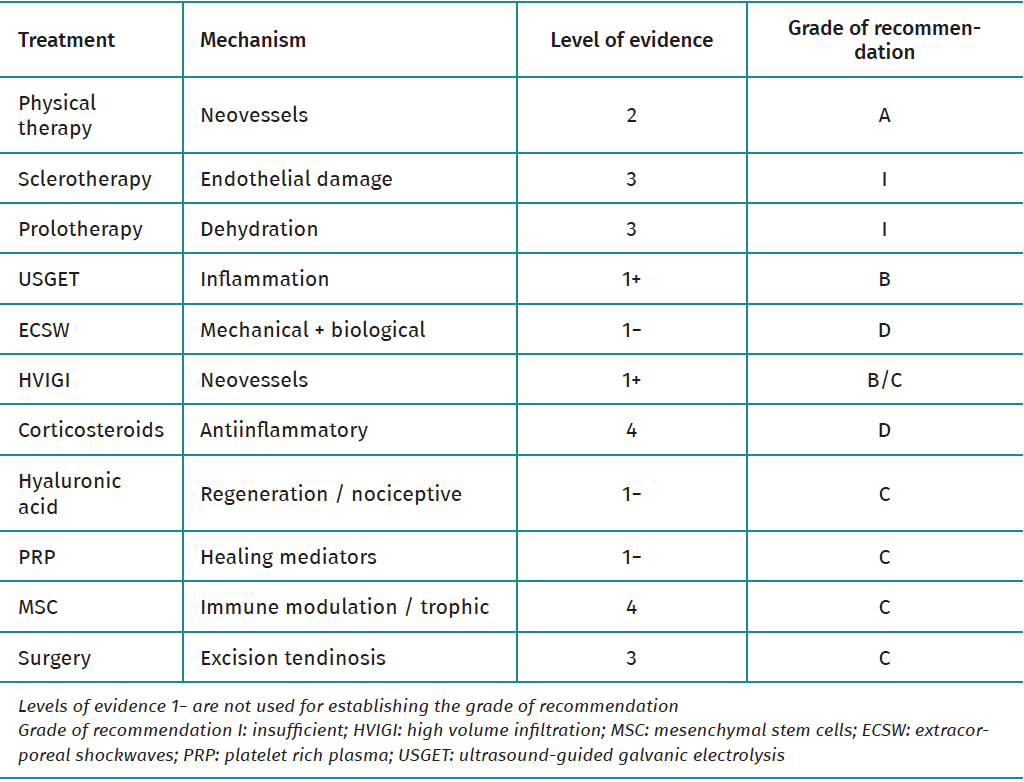
Table 1. Treatment alternatives in patellar tendinopathy.
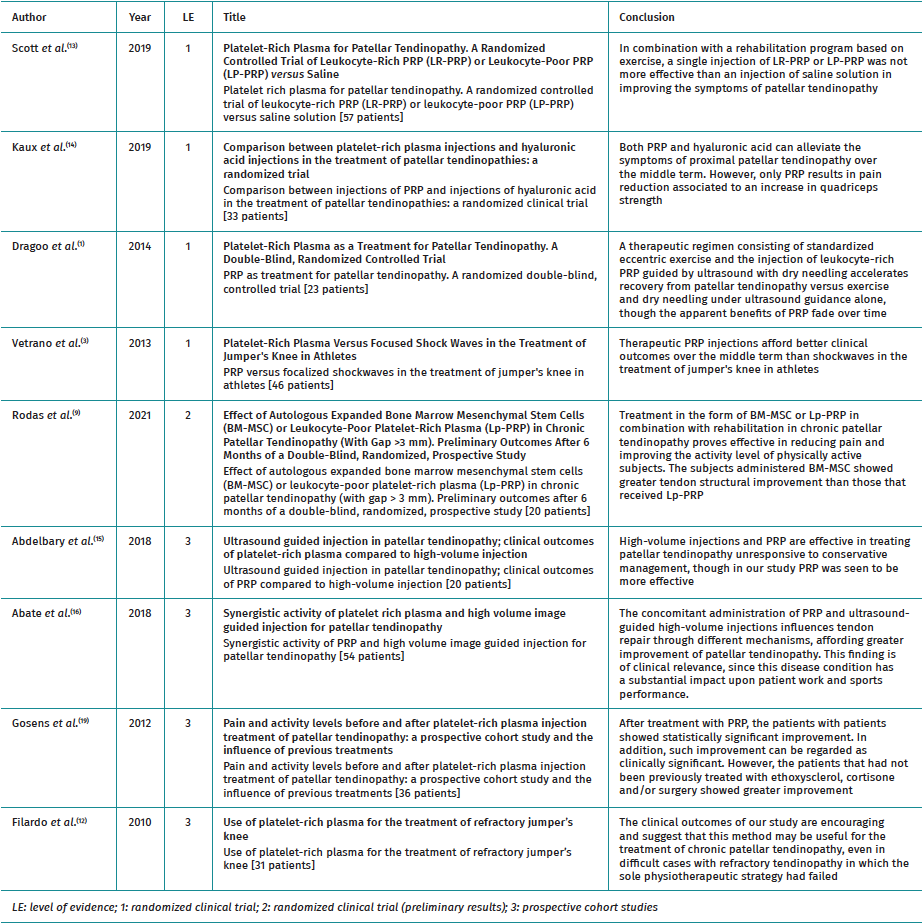
Table 2. Clinical trials and prospective cohort studies on the use of platelet rich plasma (PRP) in patellar tendinopathy.
Figuras
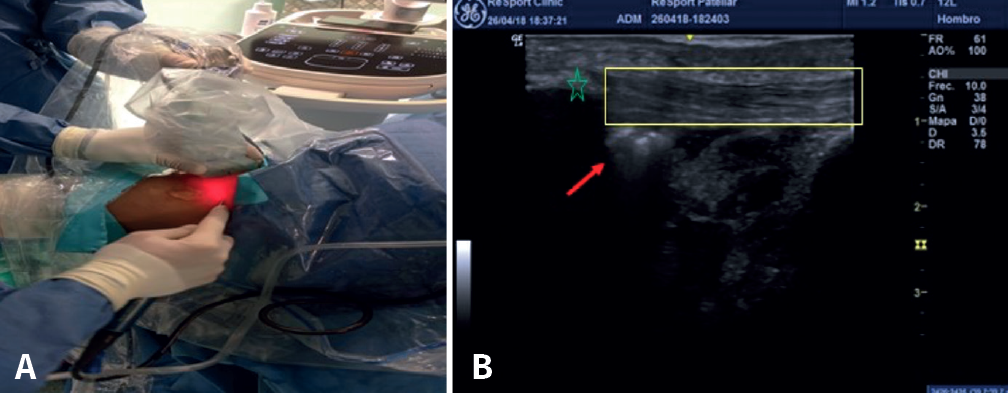
Figure 1. A: after creating the anterolateral and anteromedial knee portal 1 cm more lateral and more medial, respectively, resection is carried out of the neovessels and nerve tissue of the posterior aspect of the patellar tendon, as well as of the area of tendinosis and/or calcification in the posterior zone, until a tendon is obtained of the same thickness as the healthy contralateral tendon(74). The technique requires an assistant to hold the ultrasound device while the main surgeon controls the optics and the synoviotome. B: the red arrow indicates the location of the synoviotome over the deep zone of the patellar tendon (yellow inset). The asterisk shows the distal pole of the patella.
Información del artículo
Cita bibliográfica
Ethical responsibilities
Conflicts of interest. The authors state that they have no conflicts of interest.
Financial support. This study has received no financial support.
Protection of people and animals. The authors declare that this research has not involved human or animal experimentation.
Data confidentiality. The authors declare that the protocols of their work centre referred to the publication of patient information have been followed.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
Descargar artículo:
Licencia:
Este contenido es de acceso abierto (Open-Access) y se ha distribuido bajo los términos de la licencia Creative Commons CC BY-NC-ND (Reconocimiento-NoComercial-SinObraDerivada 4.0 Internacional) que permite usar, distribuir y reproducir en cualquier medio siempre que se citen a los autores y no se utilice para fines comerciales ni para hacer obras derivadas.
Comparte este contenido
En esta edición
- From the start to the top: the history of knee osteotomies
- Clinical-functional and radiographic outcomes of medial valgus-producing tibial osteotomy
- Patellar tendinopathy: a practical consensus guide for choosing the best treatment
- Evolution of spinal endoscopy. Where do we come from and where are we going?
- Partial ruptures of the rotator cuff
- Arthroscopic core decompression of the femoral head with autologous stem cell placement as treatment for femoral head osteonecrosis
- Extraarticular plasty as sole maneuver in the correction of rotational instability due to rupture of the anterior cruciate ligament in an elderly patient
- Fully arthroscopic osteosynthesis with button placement in acute anterior glenoid fracture: a case report
- Arthroscopic visualization of the popliteal hiatus and localization of an intraarticular free body
Más en PUBMED
Más en Google Scholar

Revista Española de Artroscopia y Cirugía Articular está distribuida bajo una licencia de Creative Commons Reconocimiento-NoComercial-SinObraDerivada 4.0 Internacional.