
Circumferential 270º reconstruction of the hip labrum through arthroscopy with knotless tensionable technology Surgical technique
Reconstrucción del labrum de la cadera circunferencial 270° por vía artroscópica con tecnología tensionable sin nudos. Técnica quirúrgica
Introduction
The acetabular labrum is a fibrocartilaginous structure joined to the cotyloid cavity at its periphery. It contains nerve endings that play a role in proprioception and nociception of the joint, and it contributes in an important way to hip stability and biomechanics, as well as to preservation of the joint cartilage. Likewise, it exerts a sealing effect that makes it the main stabilising mechanism against traction forces in minor displacements (1-2 mm). In addition, this sealing effect contributes to maintain an environment with a low friction coefficient, reducing stress and tension upon the joint cartilage by keeping the joint surfaces separated, and distributing the loads through the pressurised liquid layer(1,2,3,4). Based on the above, there has been an increased interest in the treatment of acetabular labrum injuries over the last decade. The surgical treatment options include debridement, resection, labral repair, augmentation and reconstruction, with the use of autografts or allografts(5,6).
Labral reconstruction using graft material is an increasingly common technique in primary and revision surgery of the hip, involving tissue implantation to also restore the joint sealing effect. Such reconstruction may be segmental or circumferential (270°). Circumferential labral reconstruction is carried out in cases characterised by extensive labral tearing, poor tissue quality, or a small and atrophic labrum. Segmental reconstruction in turn is indicated in cases characterised by a limited defect size and the existence of an altered chondrolabral junction. In the case of preservation of the chondrolabral junction in a patient with a limited defect or hypoplastic labrum, a reinforcement or augmentation technique is used, preserving the existing labrum (Figure 1).
reacae.30178.fs2209014-figure1.png
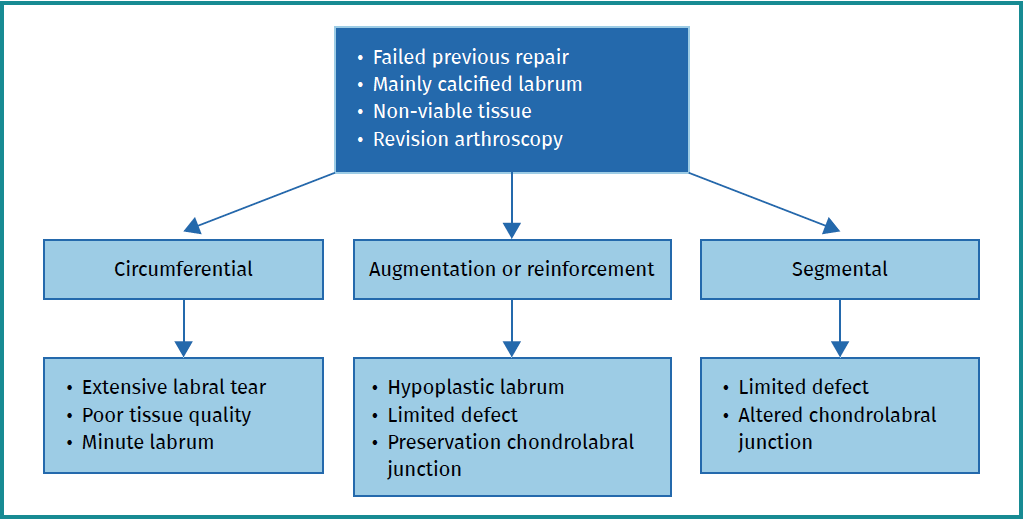
Figure 1. Indications for labral reconstruction and the recommended techniques.
The present study describes the surgical technique used for circumferential 270º reconstruction of the acetabular labrum involving tibialis anterior allografts with the use of knotless tensionable technology based on the procedure of Benjamin Domb(7,8).
Surgical technique
Diagnostic tests
The imaging diagnostic tests should include radiographs to determine whether bone procedures (osteochondroplasty or acetabuloplasty) are required or not, as well as magnetic resonance imaging (MRI) to visualise or reveal areas of degeneration / re-rupture / adherences in the acetabular labrum resulting in a possible loss of joint sealing, where suturing proves very difficult or impossible. The technique is not indicated in cases of advanced joint damage.
Positioning
Under combined (spinal and general) anaesthesia, the patient is placed on the traction table in supine decubitus with the contralateral leg in abduction. The hip to be operated upon is placed in 10-15º flexion and is moved towards the neutral midline (Figure 2). The hip is distracted through longitudinal traction combined with the pressure of a perineal post. The foot of the leg to be operated upon is rotated internally to move the femoral neck parallel to the floor, and the table is inclined 10º towards the opposite side(9). Under conditions of asepsis and antisepsis, the surgical field is prepared, and the anatomical references are marked: anterosuperior iliac spine, trochanter and longitudinal line from the spine to the centre of the patella, which determines the safe zone for working, avoiding the risk of vascular and nerve damage.
reacae.30178.fs2209014-figure2.png
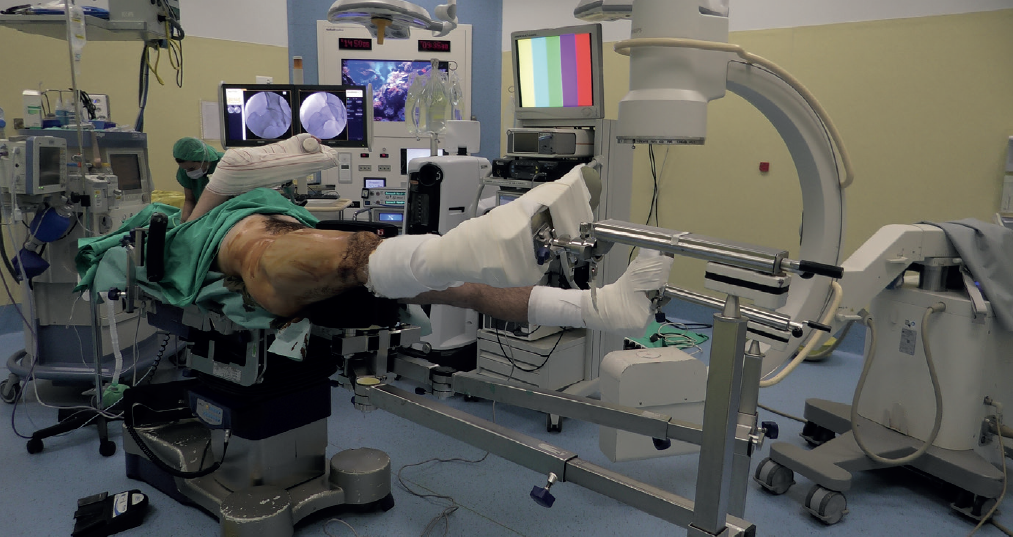
Figure 2. Image of the patient placed in supine decubitus on the traction table. The hip to be operated upon (in this case the right hip) is placed in 10-15º flexion and aligned with the trunk of the patient. The foot of the leg to be operated upon is rotated internally to move the femoral neck parallel to the floor, and the table is inclined 10º towards the opposite side. The radioscopic equipment and arthroscopy tower are positioned on the opposite side.
Portals
For this technique, use is made of the modified anterior, anterolateral, medial oblique and posterolateral portals, and the all inside technique is employed with maximum capsular preservation(10) (Figures 3 and 4).
reacae.30178.fs2209014-figure3.png
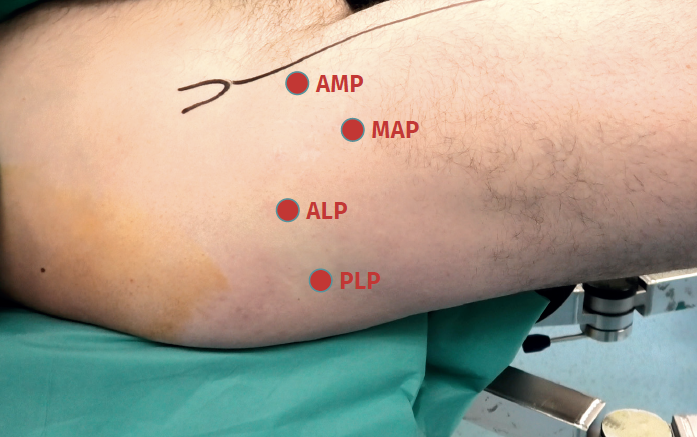
Figure 3. Labral reconstruction portals. Right hip. Anterolateral portal (ALP). Location: upper margin of the greater trochanter in line with its anterior margin or 1 cm anterior and 1 cm superior to the tip of the greater trochanter. Insertion angle: 10-15° in the cephalic direction and 10-15° of posterior inclination. Modified anterior portal (AMP): at the same height as the anterolateral portal and 1 cm lateral to the longitudinal line from the anterosuperior iliac spin to the centre of the patella. Medial oblique portal (MAP): located 6-7 cm distal to the anterolateral portal, at an angle of about 45-60º. Posterolateral portal (PLP): Location: upper margin of the greater trochanter in line with its posterior margin or 1 cm posterior and 1 cm superior to the tip of the greater trochanter.
- Anterolateral portal. Location: upper margin of the greater trochanter in line with its anterior margin or 1 cm anterior and 1 cm superior to the tip of the greater trochanter. Insertion angle: 10-15° in the cephalic direction and 10-15° of posterior inclination.
- Modified anterior portal. At the same height as the anterolateral portal and 1 cm lateral to the longitudinal line from the anterosuperior iliac spin to the centre of the patella.
- Medial oblique portal. Located 6-7 cm distal to the anterolateral portal, at an angle of about 45-60º.
- Posterolateral portal. Location: upper margin of the greater trochanter in line with its posterior margin or 1 cm posterior and 1 cm superior to the tip of the greater trochanter.
reacae.30178.fs2209014-figure4.png
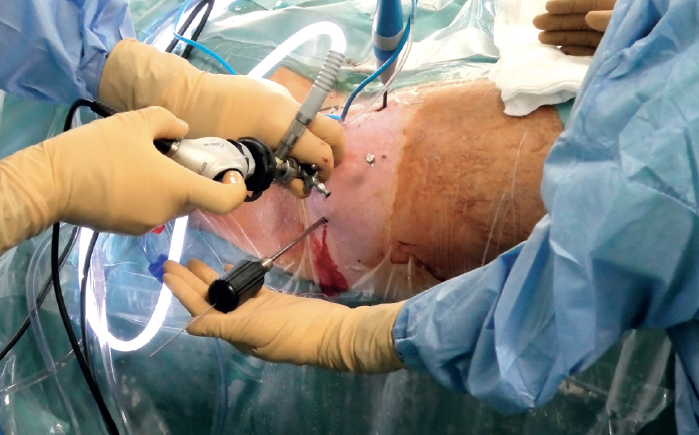
Figure 4. Portals. Right hip. Camera in the anterolateral portal. Radiofrequency in the modified anterior portal. Needle in the medial oblique portal. Dilator in the posterolateral portal.
Arthroscopy, labral check and preparation or the acetabulum
Once the anterolateral and modified anterior portals have been established, an interportal capsulotomy is performed to allow handling of the instruments within the joint. During the procedure a degenerated labrum is observed, with re-ruptures and adherences, and the segment is removed over a circumferential area from the 4 o'clock position anterior, superior and posterior to the 8 o'clock position (Figure 5). Levelling of the residual hump (if any) is carried out, and acetabuloplasty is performed with motor-driven instruments based on the usual technique, and under fluoroscopic and arthroscopic control.
reacae.30178.fs2209014-figure5.png

Figure 5. Illustration of circumferential 270º reconstruction of the acetabular labrum. In a right hip, the procedure would extend from the 4 o'clock position anterior, then superior, and would end posterior at about 8 o'clock.
Preparation of the graft
For this procedure, use is made of an tibialis anterior allograft that is cut and prepared to obtain a diameter of 6-7 mm and a length of about 18 cm. Using FiberLoop® suture, the extremities are prepared with the SpeedWhip® (Arthrex) technique, and the anterior part is marked (Figure 6).
reacae.30178.fs2209014-figure6.png

Figure 6. Preparation of the tibialis anterior allograft: the graft is cut and prepared to obtain a diameter of 6-7 mm and a length of about 18 cm. Using FiberLoop® suture, the extremities are prepared with the SpeedWhip® technique.
Pre-drilling and placement of acetabular anchorings
From the modified anterior portal, pre-drilling is performed at the 4 o'clock position (Figure 7) to implant an anchoring, with two possible variants: PressFT® 2.8 mm (Conmed), or an all-filament anchoring followed by threading of the extremity. Then, and also through the modified anterior portal or from the medial oblique portal, the first FiberTAK® Knotless 1.8 mm tensioning (Arthrex) anchoring is positioned 1 cm from the most anterior pre-drilling or anchoring, and its filaments are retrieved through the medial oblique portal. The successive FiberTAK® Knotless sutures are introduced through the medial oblique portal until reaching the posterior zone at the 8 o'clock position (Figures 8 and 9). During perforation and pre-drilling of the anchoring, the arthroscope is to be placed in a position allowing assessment of the joint cartilage, in order to make sure that the drill is not located between the subchondral bone and the surface of the joint cartilage. In order to prevent the anchorings from penetrating into the acetabular cartilage, the angle of the margin must be determined to ensure adequate placement. Lastly, the most posterior anchoring is introduced through the posterolateral portal and is also retrieved through the medial oblique portal. The successive filaments are placed in the field aligned and spread out in a fan-like manner from inferior-anterior to posterior-superior (Figures 10 and 11).
reacae.30178.fs2209014-figure7.png
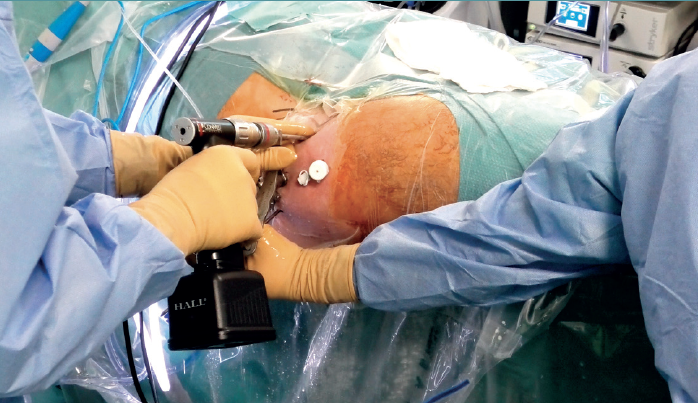
Figure 7. Right hip. Exterior anterior pre-drilling view from the modified anterior portal at the 4 o'clock position. Camera in the anterolateral portal. Cannula in the medial oblique portal.
Insertion of the graft
Forceps are inserted from the posterior portal, taking care that they lie posterior to the last anchoring, and from the anterior modified portal we introduce the suture anchored to the anterior portion of the graft, likewise taking care that it lies anterior to the most anterior anchoring. Once within the joint, this suture is grasped with the forceps inserted from the posterior portal, and then traction is exerted posterior until it emerges from the posterolateral portal. Lastly, traction is continued to introduce the graft, making it emerge through the posterolateral portal. At this point, the anchoring preassembled in the graft is guided towards the pre-drilling made and is inserted, thereby fixing the most anterior portion of the graft in the case of using a knotless anchoring or extracting the suture and threading the tendon to then perform a knotted technique(Figure 12). After positioning and fixation of the most anterior portion of the graft, the filaments are passed around the graft in sequence, and are tightened little by little, maintaining traction from the posterolateral portal, and fixing and positioning the entire plasty from anterior to posterior (Figures 13 and 14). Once all these steps have been completed, the excess graft is radiofrequency amputated from the posterolateral portal. Lastly, the hip is evaluated dynamically in all the planes of motion, checking fixation, the position of the graft, and recreation of the sealing effect at the femoral head-neck junction with the acetabular labrum (Figure 15).
reacae.30178.fs2209014-figure8.png
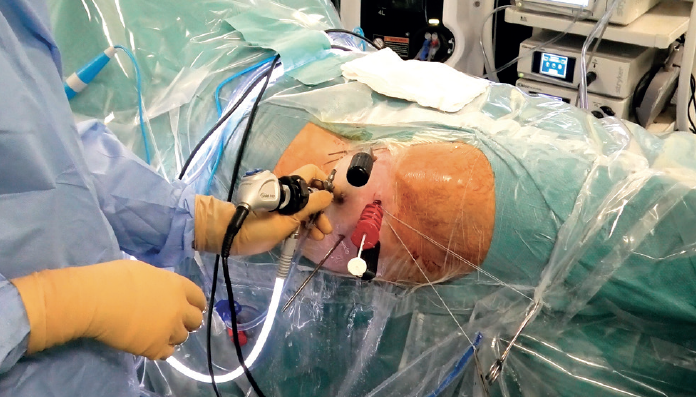
Figure 8. Introduction of FiberTAK® Knotless 1.8 mm sutures through the medial oblique portal with tensionable technology (Arthrex).
Finally, capsule closure is carried out using the routine technique. Table 1 describes the advantages and limitations of the procedure, and Table 2 indicates the key points to be taken into account.
reacae.30178.fs2209014-figure9.png
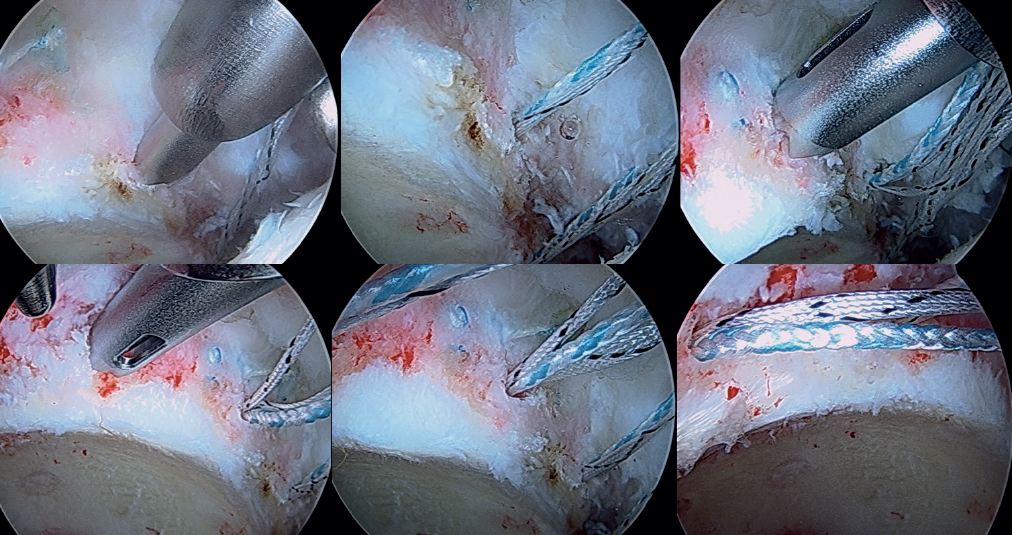
Figure 9. Arthroscopic view of drilling and placement of the anchorings in the anterosuperior zone.
Postoperative rehabilitation
The patient is discharged the day after surgery and follows the usual postoperative rehabilitation for labral repair and decompression due to femoroacetabular impingement, with weight bearing assisted by crutches and circumduction movements and static bicycling during 6 weeks. The patient is to avoid abduction in excess of 20º, extension, and flexion is to be limited to 80-90º during two months. Physical activity begins after three months, and after about 6 months a gradual return to sports activity is allowed.
reacae.30178.fs2209014-figure10.png

Figure 10. The most posterior anchoring is introduced through the posterolateral portal and is also retrieved through the medial oblique portal. The successive filaments are placed in the field aligned and spread out in a fan-like manner from inferior-anterior to posterior-superior.
Discussion
Although repair is the gold standard for the primary treatment of labral injuries, circumferential or segmental reconstruction is more commonly performed in revision surgery. The main indications for reconstruction are: a non-reparable labrum, of poor quality, insufficient (< 2 mm), hypertrophic and dysfunctional (> 8 mm) or calcified, in a patient without osteoarthrosis or with only minimal osteoarthrosis(5,6,11,12,13).
reacae.30178.fs2209014-figure11.png
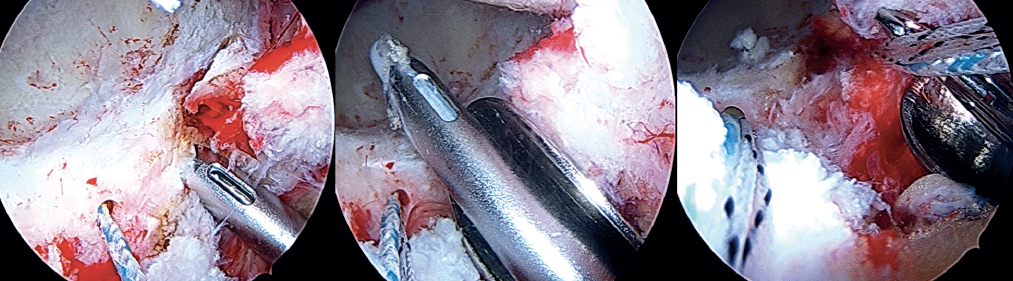
Figure 11. Arthroscopic view of drilling and placement of the most posterior anchorings at the 8 o'clock position.
Philippon et al. first described the technique for arthroscopic reconstruction of the acetabular labrum using iliotibial band grafting in 2010. This study of 47 patients reported good outcomes over 18 months of follow-up(14). A range of allografts have been proposed and described in the literature. The advantages of using an allograft include lesser morbidity at the patient donor site, as well as control of the thickness and length of the graft. Furthermore, as this is non-innervated tissue, the possibility of graft-related postoperative pain decreases(13,15).
reacae.30178.fs2209014-figure12.png
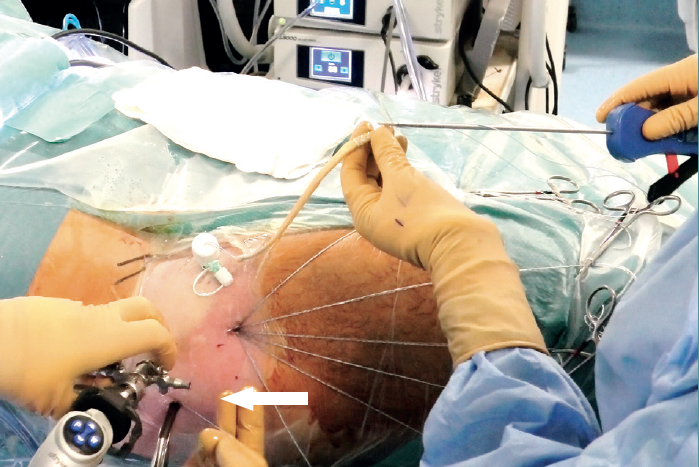
Figure 12. External view showing displacement of the anchoring preassembled in the graft towards the anterior pre-drilling site at the 4 o'clock position, which is then inserted to thus fix the most anterior part of the reconstruction. The arrow indicates the traction suture in the posterolateral portal, which will be used for traction and to introduce the graft, making it emerge through the posterolateral portal.
The acetabular labrum plays a very important role in the stability and good functioning of the hip. Philippon et al. recorded a 47% loss in hip pressurisation in the presence of a partial lesion of the labrum, and a 76% loss in pressurisation when complete resection of the labrum was performed(2). Neppel et al. showed that on losing the suction effect in the hip, the main stabiliser in displacements of over 2 mm is lost(3). In addition, Kapetanakis et al. recorded significant differences in the histological structure of the acetabular labrum between healthy individuals and subjects with grade III and IV osteoarthritis(1).
reacae.30178.fs2209014-figure13.png
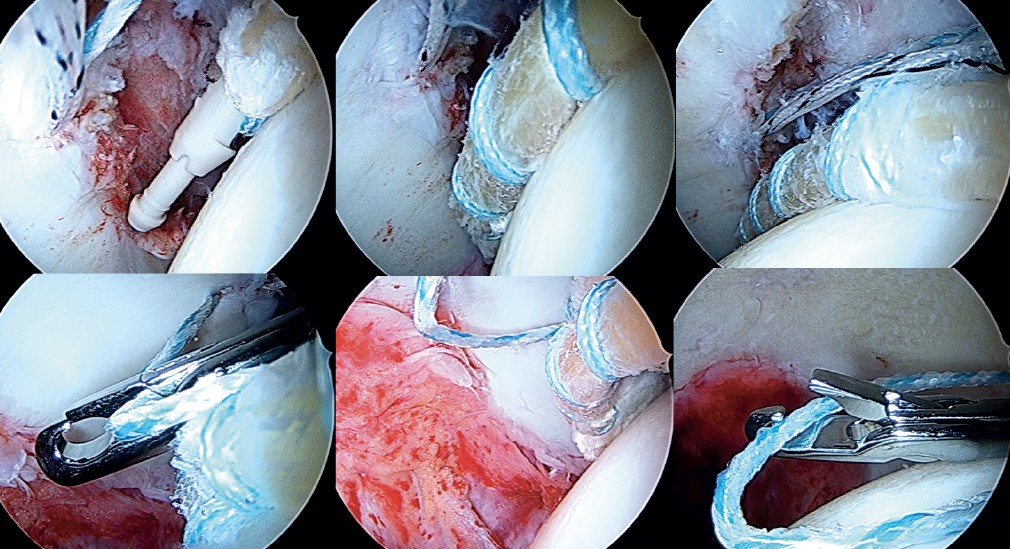
Figure 13. Arthroscopic view showing introduction and posterior fixation of the most anterior portion of the graft; the filaments are passed around the tibialis anterior in sequence, and are tightened little by little, maintaining traction from the posterolateral portal, and fixing and positioning the plasty.
Reconstruction of the acetabular labrum is an effective treatment option that can restore the biomechanical properties of the hip. Although this procedure has mainly been described as revision surgery, in recent years it has been increasingly proposed as primary surgery in patients with a non-reparable or insufficient labrum(16). Scanaliato et al. compared results between patients subjected to labrum repair and patients undergoing circumferential reconstruction of the labrum as primary procedure. The follow-up period was two years, and the results were equally satisfactory in the labrum repair group and in the primary reconstruction group(17). With regard to the choice of graft, no significant differences have been demonstrated between autografts and allografts. However, due to the lesser morbidity related to the patient donor site and to the shorter surgery time involved, we lately prefer to use allografts. The anterior / posterior tibialis tendon is very convenient for this technique due to its shape, length and thickness(18,19). Moya et al. published a series of 20 reconstructions of the acetabular labrum with allografts, obtaining good to excellent outcomes over an average follow-up of 5 years(20).
reacae.30178.fs2209014-figure14.png
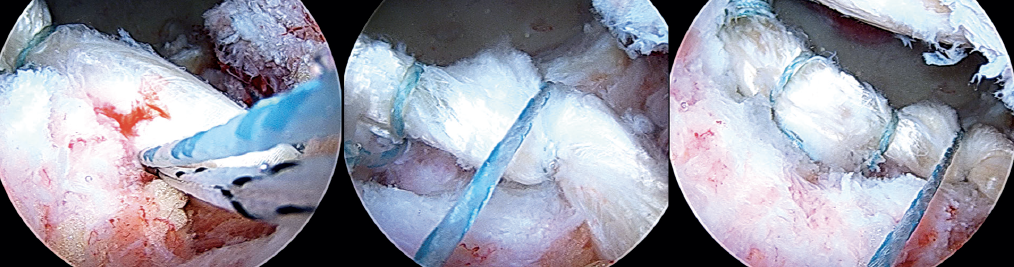
Figure 14. Arthroscopic view showing handling of the sutures in the most posterior part of the acetabulum at the 8 o'clock position.
Arthroscopic reconstruction of the acetabular labrum is a technically demanding procedure with an important learning curve. In this respect, the surgeon may have great experience in hip arthroscopy but feel inexperienced in reconstruction of the labrum(15). Of the different acetabular labrum reconstruction techniques available, no single procedure has been shown to be superior to the rest(13). The "forward-backward" technique described by White and Herzog(21) requires measurement with a graft oversized by about 2 cm in order to avoid it from being too short. In 2017, Domb et al. published their knotless pull-through technique, which offered the advantage of obviating precise measurements, since the use of a graft of surplus length implied that the excess graft could be amputated after fixation(7). The outcomes of this technique over two years of follow-up demonstrate its efficacy(8).
reacae.30178.fs2209014-figure15.png
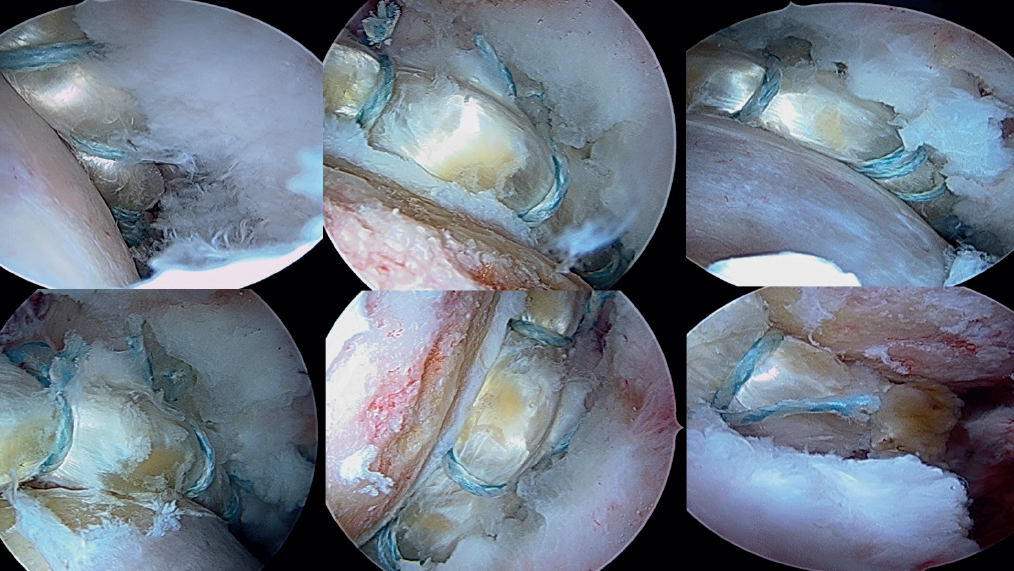
Figure 15. Arthroscopic view showing dynamic evaluation of the hip in all the planes of motion, checking fixation, the position of the graft, and recreation of the sealing effect at the femoral head-neck junction with the implanted labrum graft.
With the recent rise in the use of arthroscopy in application to the hip, the revision rates due to inadequate outcomes has increased. The management of these patients with residual pain and recurrent symptoms is a challenge as far as diagnosis and treatment are concerned. Recently, specific techniques have been developed that are usually only used in revision scenarios such as labral reconstruction. In cases characterised by great labral involvement, circumferential 270º reconstruction of the labrum appears to be the most appropriate technique for dealing with this problem. The use of a tibialis anterior tendon allograft adds the advantage that no prior measurement is needed to see the required length of graft. The use of knotless tensionable technology facilitates performance of this complex technique.
reacae.30178.fs2209014-table1.png
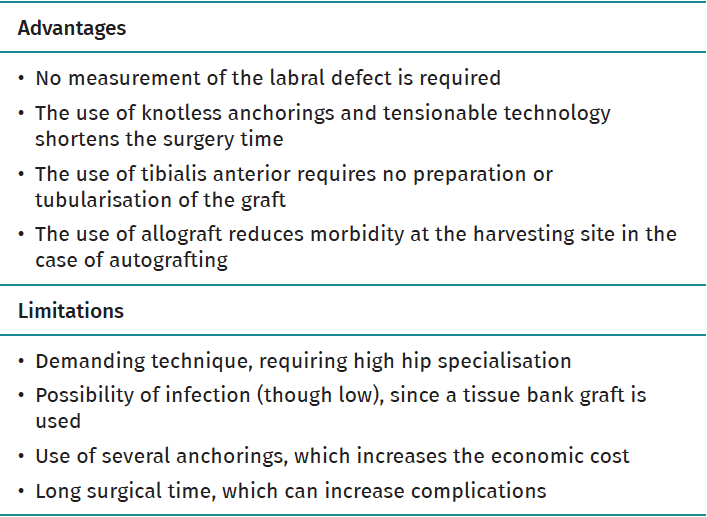
Table 1. Advantages and limitations
reacae.30178.fs2209014-table2.png
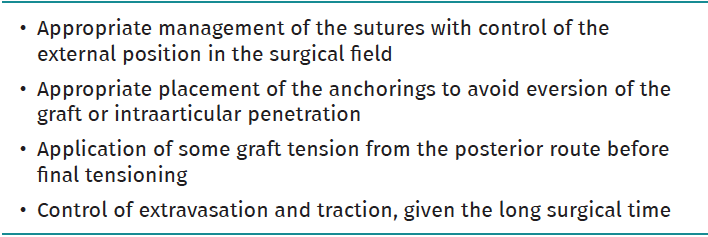
Table 2. Key points be taken into account
Conclusion
Circumferential reconstruction of the acetabular labrum in a young patient with complete absence of labral function and with high performance demands, with recurrent pain after hip arthroscopy, is a surgical option for preserving the physiological integrity of the hip joint. The technique is complex and must be performed by surgeons with a large volume of surgeries of this kind.
Supplementary material (Video 1)
Video 1. Circumferential 270º reconstruction of the hip labrum through arthroscopy with knotless tensionable technology.
Figuras
Figure 1. Indications for labral reconstruction and the recommended techniques.
Figure 2. Image of the patient placed in supine decubitus on the traction table. The hip to be operated upon (in this case the right hip) is placed in 10-15º flexion and aligned with the trunk of the patient. The foot of the leg to be operated upon is rotated internally to move the femoral neck parallel to the floor, and the table is inclined 10º towards the opposite side. The radioscopic equipment and arthroscopy tower are positioned on the opposite side.
Figure 3. Labral reconstruction portals. Right hip. Anterolateral portal (ALP). Location: upper margin of the greater trochanter in line with its anterior margin or 1 cm anterior and 1 cm superior to the tip of the greater trochanter. Insertion angle: 10-15° in the cephalic direction and 10-15° of posterior inclination. Modified anterior portal (AMP): at the same height as the anterolateral portal and 1 cm lateral to the longitudinal line from the anterosuperior iliac spin to the centre of the patella. Medial oblique portal (MAP): located 6-7 cm distal to the anterolateral portal, at an angle of about 45-60º. Posterolateral portal (PLP): Location: upper margin of the greater trochanter in line with its posterior margin or 1 cm posterior and 1 cm superior to the tip of the greater trochanter.
Figure 4. Portals. Right hip. Camera in the anterolateral portal. Radiofrequency in the modified anterior portal. Needle in the medial oblique portal. Dilator in the posterolateral portal.
Figure 5. Illustration of circumferential 270º reconstruction of the acetabular labrum. In a right hip, the procedure would extend from the 4 o'clock position anterior, then superior, and would end posterior at about 8 o'clock.
Figure 6. Preparation of the tibialis anterior allograft: the graft is cut and prepared to obtain a diameter of 6-7 mm and a length of about 18 cm. Using FiberLoop® suture, the extremities are prepared with the SpeedWhip® technique.
Figure 7. Right hip. Exterior anterior pre-drilling view from the modified anterior portal at the 4 o'clock position. Camera in the anterolateral portal. Cannula in the medial oblique portal.
Figure 8. Introduction of FiberTAK® Knotless 1.8 mm sutures through the medial oblique portal with tensionable technology (Arthrex).
Figure 9. Arthroscopic view of drilling and placement of the anchorings in the anterosuperior zone.
Figure 10. The most posterior anchoring is introduced through the posterolateral portal and is also retrieved through the medial oblique portal. The successive filaments are placed in the field aligned and spread out in a fan-like manner from inferior-anterior to posterior-superior.
Figure 11. Arthroscopic view of drilling and placement of the most posterior anchorings at the 8 o'clock position.
Figure 12. External view showing displacement of the anchoring preassembled in the graft towards the anterior pre-drilling site at the 4 o'clock position, which is then inserted to thus fix the most anterior part of the reconstruction. The arrow indicates the traction suture in the posterolateral portal, which will be used for traction and to introduce the graft, making it emerge through the posterolateral portal.
Figure 13. Arthroscopic view showing introduction and posterior fixation of the most anterior portion of the graft; the filaments are passed around the tibialis anterior in sequence, and are tightened little by little, maintaining traction from the posterolateral portal, and fixing and positioning the plasty.
Figure 14. Arthroscopic view showing handling of the sutures in the most posterior part of the acetabulum at the 8 o'clock position.
Figure 15. Arthroscopic view showing dynamic evaluation of the hip in all the planes of motion, checking fixation, the position of the graft, and recreation of the sealing effect at the femoral head-neck junction with the implanted labrum graft.
Tablas
Table 1. Advantages and limitations
Table 2. Key points be taken into account
Información del artículo
Cita bibliográfica
Ethical responsibilities
Conflicts of interest. The authors state that they have no conflicts of interest.
Financial support. This study has received no financial support.
Protection of people and animals. The authors declare that this research has not involved human or animal experimentation.
Data confidentiality. The authors declare that the protocols of their work centre referred to the publication of patient information have been followed.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
Descargar artículo:
Licencia:
Este contenido es de acceso abierto (Open-Access) y se ha distribuido bajo los términos de la licencia Creative Commons CC BY-NC-ND (Reconocimiento-NoComercial-SinObraDerivada 4.0 Internacional) que permite usar, distribuir y reproducir en cualquier medio siempre que se citen a los autores y no se utilice para fines comerciales ni para hacer obras derivadas.
Comparte este contenido
En esta edición
- The COVID hangover
- Results of the arthroscopic treatment of acute bony Bankart lesion using the original Porcellini-Sugaya technique and the double-row modified procedure
- Assessment of tibial translation in experimental models of anterior cruciate ligament reconstructions: is dual tibial fixation indicated?
- Learning curve in the arthroscopic Latarjet technique
- Clinical outcomes of the anteromedial technique versus the transtibial technique in reconstruction of the anterior cruciate ligament: a systematic review and meta-analysis of randomized clinical trials
- Basic sciences in reconstruction of the anterior cruciate ligament with the ischiotibial tendons (a narrative review)
- Arthroscopic hip surgery in femoroacetabular impingement
- Circumferential 270º reconstruction of the hip labrum through arthroscopy with knotless tensionable technology Surgical technique
- Arthroscopic capsule reconstruction with dermal mesh plus segmental labral reconstruction with tibialis anterior allograft in recurrent postsurgical hip microinstability
- Synthetic polyethylene mesh augmentation for chronic patellar tendon rupture repair
- The Giant’s Causeway “inside the shoulder”
Más en PUBMED
Más en Google Scholar
Más en ORCID

Revista Española de Artroscopia y Cirugía Articular está distribuida bajo una licencia de Creative Commons Reconocimiento-NoComercial-SinObraDerivada 4.0 Internacional.