
Perioperative analgesia in arthroscopy of the hip
Analgesia perioperatoria en artroscopia de cadera
Introduction
Arthroscopy of the hip has grown exponentially in recent years. In England alone, the growth has been 723% in the last decade, and this figure is expected to reach 1,388% by 2023(1). Adequate postoperative pain control is crucial for improving patient satisfaction with surgery, and facilitates early mobilisation as well as the prompt start of rehabilitation(2,3). Development and improvement of the technique have made it possible to increase the number of cases in which it is carried out on an ambulatory basis. Both the percentage of patient discharge from hospital and readmission are conditioned by the management of postoperative pain. Inadequate pain management leads to delays in recovery, adverse psychological effects and an increased risk of developing chronic pain associated to the process(2). However, there is no standardised protocol for the management of perioperative pain in this surgical procedure.
The postoperative pain experienced by the patient following arthroscopy of the hip is due to a number of factors:
- Factors dependent upon the surgical technique, such as leg traction, capsule distension or fluid extravasation towards the surrounding tissues(4).
- Factors dependent upon the patient disease condition and the possible postoperative complications.
- Factors related to the psychological profile of the patient and his or her tolerance of pain(1). The presence of psychiatric disorders in patients subjected to arthroscopy of the hip due to femoroacetabular impingement appears to be quite common(5). As in other disease conditions, it is known that this can worsen the surgical outcome(6). However, there have also been promising publications in this regard, as in the study published by Zacharias(7), who recorded a decrease in psychiatric medication use in patients diagnosed with depression or anxiety at least one year before surgery.
Some intraoperative manoeuvres, such as the use of high pressures in the pump, labral repair and femoral osteochondroplasty appear to cause more pain during the postoperative phase. Utilisation of the fluid infusion pump at a pressure of 40 mmHg may result in less postoperative pain(8).
The combination of correct pre- and postoperative analgesic medication with nerve blocks appears to offer the best postoperative analgesia, reducing morphic drug use in the first hours after surgery — though the side effects of each option need to be taken into account(9,10).
Assessment of postoperative pain in arthroscopy of the hip
The assessment of postoperative pain in arthroscopy of the hip is mainly based on the visual analogue scale (VAS), since this tool is simple and easy for the patient to understand. The assessment scales specifically designed for application with arthroscopy of the hip are not useful for this assessment in question, since they do not address immediate postoperative pain but are focused on follow-up at least one month after surgery.
Another parameter often used in the literature to assess the efficacy of pain treatment in the immediate postoperative period is the reduction of opioid use in the first hours after surgery.
Preoperative pain control
The concept of preventive analgesia is increasingly important in the multimodal management of pain in surgery.
It seems that a single dose of non-steroidal anti-inflammatory drugs (NSAIDs) can reduce postoperative pain and the need for opioids in the immediate postoperative period(11,12,13). Many of the studies found in the literature use 200 or 400 mg of celecoxib one hour before surgery. In the study on the triple-phase multimodal management of pain in arthroscopy of the hip published by Kolackzko et al., the first phase comprised the administration of a single preoperative dose of 975 mg of paracetamol, 300 mg of gabapentin and 200 mg of celecoxib(3).
A very interesting study carried out by Flavio García et al. on routine practices in arthroscopy of the hip among orthopaedic surgeons in different countries evidenced the differences found in the diverse geographical settings. According to the results obtained, preventive analgesia is not commonly used by 41.3% of the surgeons. Those who do use such analgesia prescribe NSAIDs, non-opiate analgesics such as paracetamol or salicylates. In geographical terms, 68.2% of the North American surgeons prescribe preventive analgesia, versus 29.5% in Central and South America, 27.3% of the surgeons in Europe, and 23.2% of those in Asia(2). As can be seen from the findings, North American surgeons are very much aware of the importance of this measure, while in Europe — and certainly also in Spain — this is not yet so.
In our opinion, it would be of benefit to introduce preventive analgesia in our practice.
Intraoperative pain control
The type of anaesthesia used during surgery influences intra- and postoperative pain control. In this respect, the use of general anaesthesia allows for greater patient comfort and control of muscle relaxation. This is important in view of its relation to the traction force needed to distract the joint and the potential complications associated with excessive traction in order to obtain sufficient space to correctly perform the required surgery. Other important factors are the pump operating pressure and the surgery time. The greater the pressure and the longer the time, the greater the probability of fluid extravasation towards the surrounding tissues and even into the abdominal cavity. Tissue distension can cause pain, and extravasation into the abdominal cavity may even produce compression and damage to nerve structures such as the crural nerve, and generate more pain in the postoperative period(4). Neuraxial anaesthesia affords more effective postoperative analgesia, but may have other undesired effects such as delayed complete clearance of the drug, which can cause falls, and the prolongation of hospital stay — this being particularly important in processes that can be carried out on an ambulatory basis(14).
In the context of multimodal management of postoperative pain in an arthroscopy of the hip, nerve blocks, particularly peripheral nerve block, seek to ensure adequate pain control in the immediate postoperative period, attempting to reduce the use of opioid analgesics and their side effects. The nausea or vomiting induced by these drugs is a frequent cause of delay in patient discharge from the postoperative recovery room and even in discharge from hospital in the case of surgery performed on an ambulatory basis(15,16).
Nerve blocks are mostly performed immediately before anaesthesia.
The hip joint is innervated by multiple nerves, and nerve block of the entire joint is therefore complex. The anterior portion of the capsule is innervated by the obturator and femoral nerves, which fundamentally receive information from that region, thereby leaving a between-nerves plane in part of the anterosuperior quadrant. The posterior portion of the capsule in turn is innervated by articular branches of the sciatic nerve, the superior gluteal nerve, the muscular branch innervating the quadratus femoris, and the inferior gluteal nerve(1,17,18). The first two cover the posterosuperior quadrant while the last two innervate the posteroinferior quadrant. This anatomical complexity makes it very difficult to achieve complete analgesic block of the hip, since doing so would require effective block of all these nerves as well as of the lateral femoral cutaneous nerve, implicated in innervation of the skin in the area where most of the hip arthroscopy portals are located.
The interesting anatomical study carried out by Mehewx showed the largest number of mechanoreceptors and sensory fibres to be located in the superolateral portion of the capsule, followed by its anterior zone — these regions coinciding with an important percentage of the disease conditions treated by means of hip arthroscopy. However, no sensory fibres were found in the inferior or posterior portion of the capsule(19).
The most frequently described blocks are femoral nerve block, lumbar plexus block and fascia iliaca block — though there is no clear preference for one specific technique. In fact, at present there is considerable controversy regarding their use.
Femoral nerve and lumbar plexus blocks afford good pain control, but also increase certain complications — particularly a risk of falls due to the motor block, especially of the quadriceps.
A number of studies involving block procedures that include the femoral nerve have reported improvement of pain in the immediate postoperative period, with a reduction of opiate use during the same period(20,21,22) in some of them, but also with a variable percentage of quadriceps weakness as well as falls attributable to motor block of this muscle(22,23). Falls of this kind can have important consequences, such as subcapital fracture due to neck weakness following resection of a cam-type deformity(24). In fact, some studies directly disadvise blocks of this kind, on the grounds that they do not afford better analgesia than other therapies, and moreover increase the risk of complications(25,26).
Fascia iliaca block does not appear to produce the same levels of analgesia and poses an increased risk of sensory neurological damage — especially of the lateral femoral cutaneous nerve(10). If obturator nerve block is added to fascia iliaca block, the analgesia achieved improves considerably(27).
Lumbar plexus block appears to offer better analgesia than fascia iliaca block, though in addition to falls(28), it may give rise to other undesired effects secondary to penetration of the neuraxial drug into the nervous system(28,29). In any case, there is considerable variability in the different publications.
The most recent studies describe spinal erector muscle blocks(30) involving infiltration of the lateral margins of the third lumbar spinous process. Zimmerer(30) recorded improved pain control versus placebo infiltration in the first 24 hours after surgery, though opiate use in the postoperative recovery room did not decrease. Descriptions have also been made of quadratus lumborum block, which has been used for years in abdominal surgery. This technique is performed in the anterolateral portion of the fascia of the quadratus lumborum muscle, and appears to reduce opiate use in the immediate postoperative period compared with patients in which no such block is performed(31).
In the study published by Kolackzko et al., the first phase involves the administration of preoperative analgesia as a single dose, as has been described above. Then, nerve block is performed in the plane of the transversalis fascia, or quadratus lumborum block is carried out. As described by the authors, this is a purely sensory block and so causes no muscle weakness or increase in the risk of falls. Following surgery, they injected 4-5 mg of morphine into the capsule, as well as 10 cc of 0.25% bupivacaine with epinephrine in the portals. In the postoperative period, the patients received 1-2 doses of 0.5 mg of intravenous (i.v.) morphine and 1-2 tablets of 5 mg of oxycodone via the oral route (p.o.). This form of multimodal analgesia reduced patient stay in the postsurgery recovery room as well as the number of readmissions due to poor pain control, compared with the group that only underwent nerve block(3).
In this same line, Fernicola et al. propose preoperative pericapsular nerve block to achieve good pain control without the risks of the other described block techniques(32).
Local infiltration analgesia (LIA) has demonstrated its efficacy in other orthopaedic surgeries and proves effective in arthroscopy of the hip, with a lesser cost compared with nerve blocks(33). Intraoperative infiltration of the portals used during arthroscopy, pericapsular infiltration and periacetabular infiltration, used isolatedly or in combination, appear to offer adequate postoperative analgesia without the risks described for some nerve block procedures(34,35,36,37). Garner and Sardesai performed local infiltration of the portals down to the joint plane, administering 40 ml of 0.25% levobupivacaine, with better results than following fascia iliaca block(1,38). The intraarticular infiltration of morphine and clonidine also appears to lessen postoperative pain and morphic drug use in the first hours after surgery, thereby reducing the side effects of such medication and affording improved patient satisfaction with the process(13). In this study, anti-inflammatory drugs were also administered preoperatively, in the same way as in other studies commented above. Another randomised prospective study comparing lumbar plexus block versus pericapsular infiltration documented similar pain control with fewer complications(39).
In our opinion, pericapsular infiltration and infiltration of the portals used during arthroscopy affords a level of postoperative analgesia similar to that obtained with peripheral nerve blocks, though with fewer complications, and so may be regarded as a first choice in this type of procedure.
Postoperative pain control
A number of drugs have been found to be useful for the management of postoperative pain in arthroscopy of the hip: NSAIDs, analgesics (non-opiate drugs such as paracetamol, and opiates) and gabapentin and its derivatives(9,40,41).
The use of NSAIDs, especially of COX-2 inhibitors and naproxen, in patients subjected to arthroscopy of the hip appears to offer a dual benefit, since it can help to control postoperative pain and to reduce the incidence of the heterotopic calcifications that sometimes appear after this type of surgery — though the dosage, duration and impact of such treatment upon the prognosis have not been clearly established(42,43,44).
The duration of postoperative analgesic treatment is highly variable. In the study published by García, over 50% of the surgeons prolonged the duration of treatment between one and two weeks. It has been reported that approximately 25% of the patients continue to use opiates for over three months after surgery. The most important risk factor for postoperative opiate use is the preoperative administration of such drugs. A negative influence is also exerted by the use of anxiolytics, the abuse of addictive substances, morbid obesity and low back pain. Prolonged opiate consumption is associated to an increased probability of severe side effects and complications. Such consumption therefore should be avoided if possible(45), particularly considering that significant reduction of the opiate dose in the postoperative period does not seem to be related to greater patient satisfaction in terms of the sensation of pain control(37,46).
The interesting study published by Nguyen et al.(47) divided the patients according to the type of postoperative pain, defining a group of fast starters (i.e., patients with a rapid start of recovery), presenting minimum discomfort and with a desire to become involved in new activities one week after surgery, versus a group of slow starters (i.e., patients with a slow start of recovery), characterised by severe pain and important limitations. A positive correlation was found between pain at one week (VAS score) and pain at two years, as well as better results on the functional scales after two years, among the fast starters.
Rehabilitation also contributes to postoperative pain control. Most of the protocols divide the rehabilitation of patients subjected to arthroscopy of the hip into four phases. In the first phase, the fundamental objective is protection of the hip and preservation of its flexibility and mobility. Emphasis is placed on manual therapy, isometric exercises (glutes, quadriceps, ischiotibial muscles, abductors and adductors), and combined exercises of the hip and trunk(48).
Recommendations (Table 1)
reacae.29276.fs2111039en-table1.png
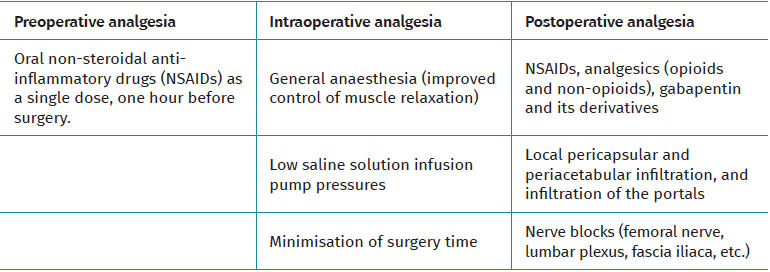
Table 1. Summary of perioperative analgesia in arthroscopy of the hip
The main elements of the proposed multimodal approach are:
- Adequate preoperative analgesia. The current tendency is to administer NSAIDs as a single dose one hour before surgery.
- Adequate intraoperative analgesia, fundamentally based on the administration of drugs, pericapsular and periacetabular local infiltrations, as well as infiltrations of the portals used during surgery. Nerve blocks (femoral nerve, lumbar plexus, fascia iliaca...) are presently more controversial for two reasons. The first reason is the complex anatomy of the innervation of the hip, which makes it difficult to achieve complete hip analgesia by means of nerve blocks, and the second reason is the risk of complications, particularly motor block, which increases the risk of falls.
- Adequate postoperative analgesia, fundamentally pharmacological. The most widely used drugs are NSAIDs, followed by analgesics (opioids and non-opioids), and gabapentin and its derivatives.
Conclusions
A multimodal management of perioperative pain in arthroscopy of the hip is clearly the best approach to secure correct pain control; patient satisfaction with the surgical procedure; lowered opiate use, with fewer side effects of such drugs; a shorter stay in the postsurgery recovery room and in hospital; and fewer readmissions due to poor pain control. The combination of correct pre- and postoperative analgesia, a careful surgical technique, periarticular and periacetabular infiltrations and infiltrations of the portals used during surgery, as well as nerve blocks, are key elements for securing good perioperative pain control. The currently most controversial aspect of these techniques is referred to nerve blocks, since these may cause motor block, especially of the quadriceps muscle, with an increased risk of falls.
Tablas
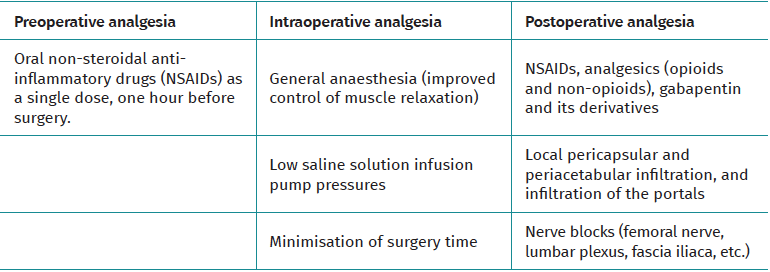
Table 1. Summary of perioperative analgesia in arthroscopy of the hip
Información del artículo
Cita bibliográfica
Ethical responsibilities
Conflicts of interest. The authors state that they have no conflicts of interest.
Financial support. This study has received no financial support.
Protection of people and animals. The authors declare that this research has not involved human or animal experimentation.
Data confidentiality. The authors declare that the protocols of their work centre referred to the publication of patient information have been followed.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
Descargar artículo:
Licencia:
Este contenido es de acceso abierto (Open-Access) y se ha distribuido bajo los términos de la licencia Creative Commons CC BY-NC-ND (Reconocimiento-NoComercial-SinObraDerivada 4.0 Internacional) que permite usar, distribuir y reproducir en cualquier medio siempre que se citen a los autores y no se utilice para fines comerciales ni para hacer obras derivadas.
Comparte este contenido
En esta edición
- The importance of pain control
- Learning from pain to make the patient feel better
- Perioperative pain management in arthroscopic surgery of the shoulder
- Perioperative pain management in arthroscopy of the elbow
- Perioperative analgesia in arthroscopic surgery of the wrist and hand
- Perioperative analgesia in arthroscopy of the hip
- Perioperative analgesia in arthroscopic surgery of the knee
- Perioperative pain management in arthroscopy of the ankle
- Postoperative neuropathic pain in traumatology
- Capsaicin 179 mg patch application technique
- Type 3 SLAP: bucket handle tear
Más en PUBMED
Más en Google Scholar
Más en ORCID

Revista Española de Artroscopia y Cirugía Articular está distribuida bajo una licencia de Creative Commons Reconocimiento-NoComercial-SinObraDerivada 4.0 Internacional.